Division of Clinical Pharmacology, Cincinnati Children's Hospital Medical Center, Cincinnati, OH.
Department of Pediatrics, University of Cincinnati College of Medicine, Cincinnati, OH.
Blood Adv. 2022 Mar 8;6(5):1454-1463. doi: 10.1182/bloodadvances.2021006523.
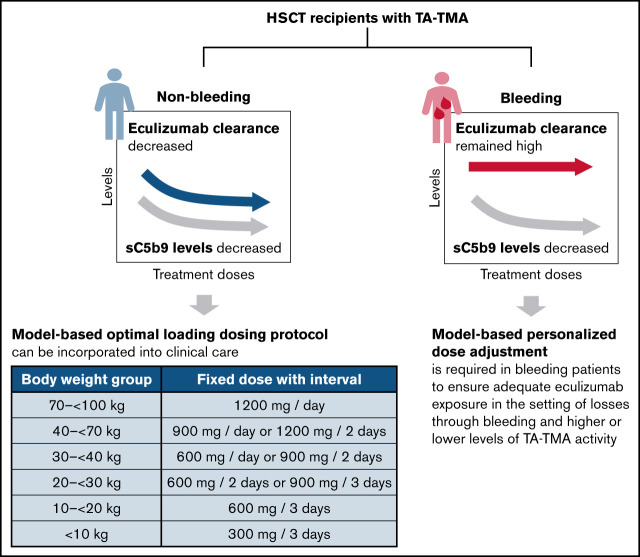
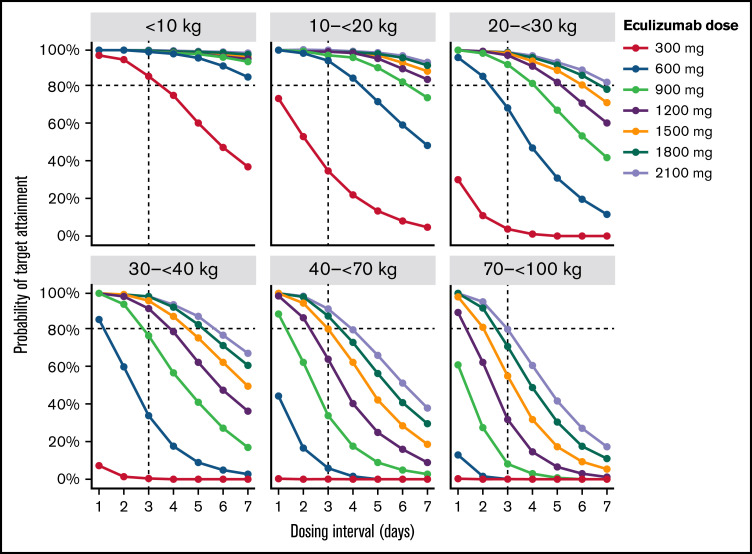
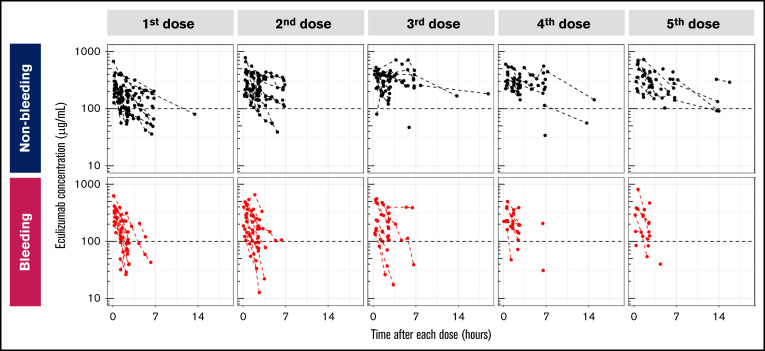
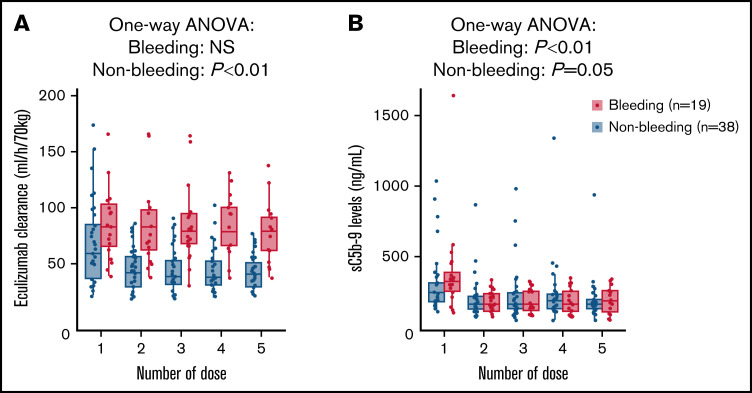
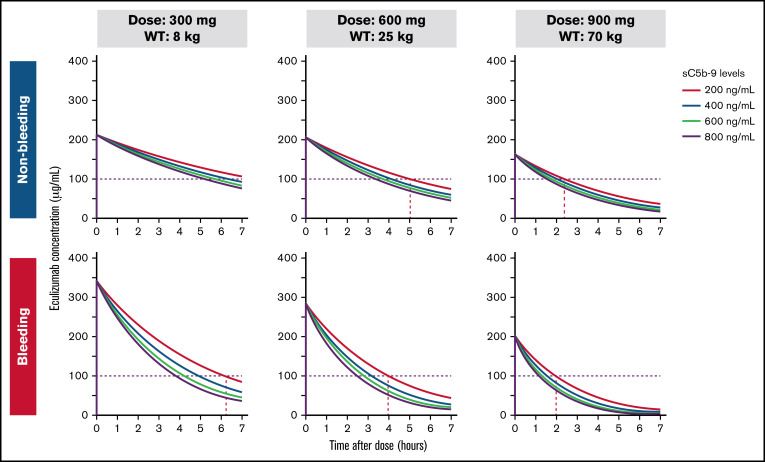
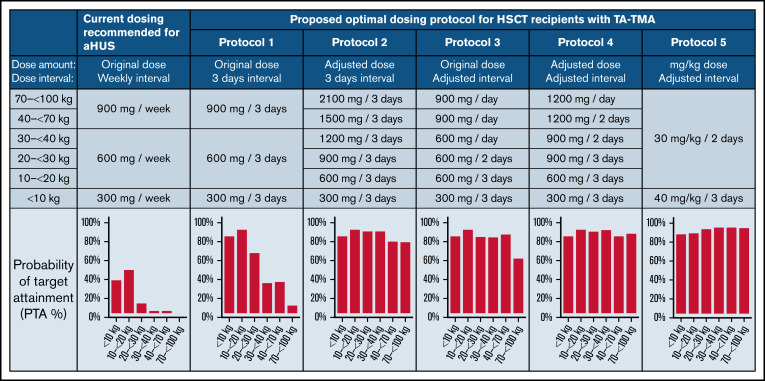
Transplant-associated thrombotic microangiopathy (TA-TMA) is a fatal posttransplant complication of hematopoietic stem cell transplantation. We recently reported that survival for TA-TMA has been improved by early intervention with eculizumab, a complement C5 inhibitor, guided by pharmacokinetic/pharmacodynamic (PK/PD) model-informed precision dosing. However, patients with gastrointestinal bleeding showed poor survival, even when treated with more frequent doses. Our objective was to develop separate models in bleeding and nonbleeding patients with TA-TMA and to propose precision dosing algorithms. Eculizumab PK/PD was analyzed in 19 bleeding and 38 nonbleeding patients (0.5-29.9 years of age). A complement activation biomarker (sC5b-9) and body weight were identified as significant determinants of eculizumab clearance regardless of bleeding. Eculizumab clearance after the first dose was higher in bleeding than in nonbleeding patients (83.8 vs 61.3 mL/h per 70 kg; P = .07). The high clearance was maintained over treatment doses in bleeding patients, whereas nonbleeding patients showed a time-dependent decrease in clearance. sC5b-9 levels were highest before the first dose and decreased over time, regardless of bleeding complications. A Monte Carlo Simulation analysis showed that the current dosing protocols recommended for atypical hemolytic uremic syndrome had <15% probability of attaining the target concentration of >100 μg/mL eculizumab in nonbleeding patients. We identified an intensified loading protocol to reach 80% target attainment. Our data clearly showed the need for individualized dosing for patients with significant bleeding and for ongoing dose adjustments to optimize outcomes. The developed models will be incorporated into a clinical decision guideline for precision dosing to improve outcomes in children and young adults with TA-TMA.
移植相关血栓性微血管病(TA-TMA)是造血干细胞移植后的一种致命的移植后并发症。我们最近报道,通过根据药代动力学/药效学(PK/PD)模型指导的精准剂量调整,早期使用补体 C5 抑制剂依库珠单抗治疗,可以改善 TA-TMA 的存活率。然而,即使接受更频繁的剂量治疗,有胃肠道出血的患者的存活率仍然很差。我们的目标是为有 TA-TMA 的出血和非出血患者分别建立模型,并提出精准剂量调整算法。分析了 19 例出血患者和 38 例非出血患者(0.5-29.9 岁)的依库珠单抗 PK/PD。无论是否有出血,补体激活生物标志物(sC5b-9)和体重均被确定为影响依库珠单抗清除率的重要决定因素。与非出血患者相比,出血患者的首次剂量后依库珠单抗清除率更高(83.8 比 61.3 mL/h/70 kg;P =.07)。在出血患者中,高清除率在治疗剂量期间得以维持,而非出血患者则表现出清除率随时间的依赖性下降。无论是否有出血并发症,sC5b-9 水平在首次剂量前最高,并随时间降低。蒙特卡罗模拟分析显示,目前推荐用于非典型溶血尿毒症综合征的剂量方案,在非出血患者中达到 >100 μg/mL 依库珠单抗目标浓度的概率<15%。我们确定了一种强化的负荷剂量方案,以达到 80%的目标达成率。我们的数据清楚地表明,对于有明显出血的患者需要个体化给药,并需要不断调整剂量以优化结果。所开发的模型将被纳入精准剂量临床决策指南,以改善 TA-TMA 儿童和青少年的治疗结果。