School of Public Health, University of the Witwatersrand, Johannesburg, South Africa.
School of Global and Public Health, Kamuzu University of Health Sciences, Blantyre, Malawi.
BMC Med Res Methodol. 2022 Jan 20;22(1):24. doi: 10.1186/s12874-021-01475-8.
In preventive drug trials such as intermittent preventive treatment for malaria prevention during pregnancy (IPTp), where there is repeated treatment administration, recurrence of adverse events (AEs) is expected. Challenges in modelling the risk of the AEs include accounting for time-to-AE and within-patient-correlation, beyond the conventional methods. The correlation comes from two sources; (a) individual patient unobserved heterogeneity (i.e. frailty) and (b) the dependence between AEs characterised by time-dependent treatment effects. Potential AE-dependence can be modelled via time-dependent treatment effects, event-specific baseline and event-specific random effect, while heterogeneity can be modelled via subject-specific random effect. Methods that can improve the estimation of both the unobserved heterogeneity and treatment effects can be useful in understanding the evolution of risk of AEs, especially in preventive trials where time-dependent treatment effect is expected.
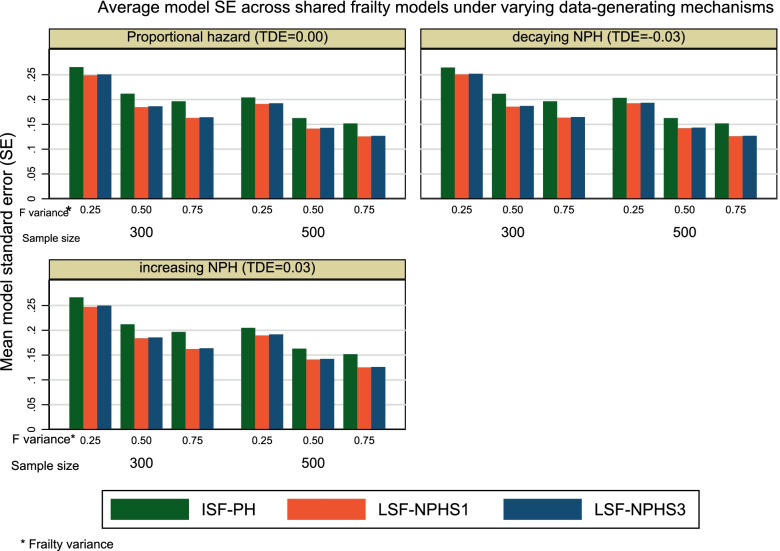
Using both a simulation study and the Chloroquine for Malaria in Pregnancy (NCT01443130) trial data to demonstrate the application of the models, we investigated whether the lognormal shared frailty models with restricted cubic splines and non-proportional hazards (LSF-NPH) assumption can improve estimates for both frailty variance and treatment effect compared to the conventional inverse Gaussian shared frailty model with proportional hazard (ISF-PH), in the presence of time-dependent treatment effects and unobserved patient heterogeneity. We assessed the bias, precision gain and coverage probability of 95% confidence interval of the frailty variance estimates for the models under varying known unobserved heterogeneity, sample sizes and time-dependent effects.
The ISF-PH model provided a better coverage probability of 95% confidence interval, less bias and less precise frailty variance estimates compared to the LSF-NPH models. The LSF-NPH models yielded unbiased hazard ratio estimates at the expense of imprecision and high mean square error compared to the ISF-PH model.
The choice of the shared frailty model for the recurrent AEs analysis should be driven by the study objective. Using the LSF-NPH models is appropriate if unbiased hazard ratio estimation is of primary interest in the presence of time-dependent treatment effects. However, ISF-PH model is appropriate if unbiased frailty variance estimation is of primary interest.
ClinicalTrials.gov; NCT01443130.
在预防药物试验中,如妊娠期间间歇性预防治疗疟疾(IPTp),存在反复治疗,预计会出现不良事件(AE)的复发。在建模 AE 风险时,面临的挑战包括考虑到 AE 发生的时间和患者内在相关性,而不仅仅是传统方法。这种相关性来自两个来源:(a)个体患者未观察到的异质性(即脆弱性)和(b)AE 之间的依赖性,这由时间相关的治疗效果来描述。潜在的 AE 依赖性可以通过时间相关的治疗效果、特定事件的基线和特定事件的随机效应来建模,而异质性可以通过特定于个体的随机效应来建模。能够改善未观察到的异质性和治疗效果估计的方法在理解 AE 风险的演变方面可能非常有用,尤其是在预期存在时间相关治疗效果的预防试验中。
我们使用模拟研究和氯喹治疗妊娠疟疾(NCT01443130)试验数据来展示模型的应用,以研究在存在时间相关治疗效果和未观察到的患者异质性的情况下,与具有比例风险的传统正态共享方差模型(ISF-PH)相比,对数正态共享方差模型是否可以改善对脆弱性方差和治疗效果的估计,这些模型带有受限三次样条和非比例风险(LSF-NPH)假设。我们根据已知的未观察到的异质性、样本量和时间相关效应的不同,评估了模型的脆弱性方差估计的偏差、精度增益和 95%置信区间的覆盖概率。
与 LSF-NPH 模型相比,ISF-PH 模型提供了更好的 95%置信区间覆盖概率,更少的偏差和更精确的脆弱性方差估计。与 ISF-PH 模型相比,LSF-NPH 模型在牺牲不精确性和高均方误差的情况下,产生了无偏差的危险比估计。
在分析复发性 AE 时,选择共享方差模型应取决于研究目标。如果在存在时间相关治疗效果的情况下,主要关注无偏危险比估计,则使用 LSF-NPH 模型是合适的。然而,如果主要关注无偏脆弱性方差估计,则 ISF-PH 模型是合适的。
ClinicalTrials.gov;NCT01443130。