Division B, Department of Medicine, University Hospital Southampton NHS Foundation Trust, Southampton General Hospital, Southampton SO16 6YD, UK.
Division B, Department of Medicine, University Hospital Southampton NHS Foundation Trust, Southampton General Hospital, Southampton SO16 6YD, UK; UHS Digital, University Hospital Southampton NHS Foundation Trust, Southampton, UK.
J Infect. 2022 Apr;84(4):558-565. doi: 10.1016/j.jinf.2022.01.034. Epub 2022 Jan 31.
Risk of hospital-acquired COVID-19 (HA-COVID-19) infection is increased by cohorting infected and non-infected patients together in assessment areas, whist awaiting laboratory PCR results. Molecular point-of-care tests (mPOCT) reduce time to results and improve patient flow but the impact on HA-COVID-19 is unknown.
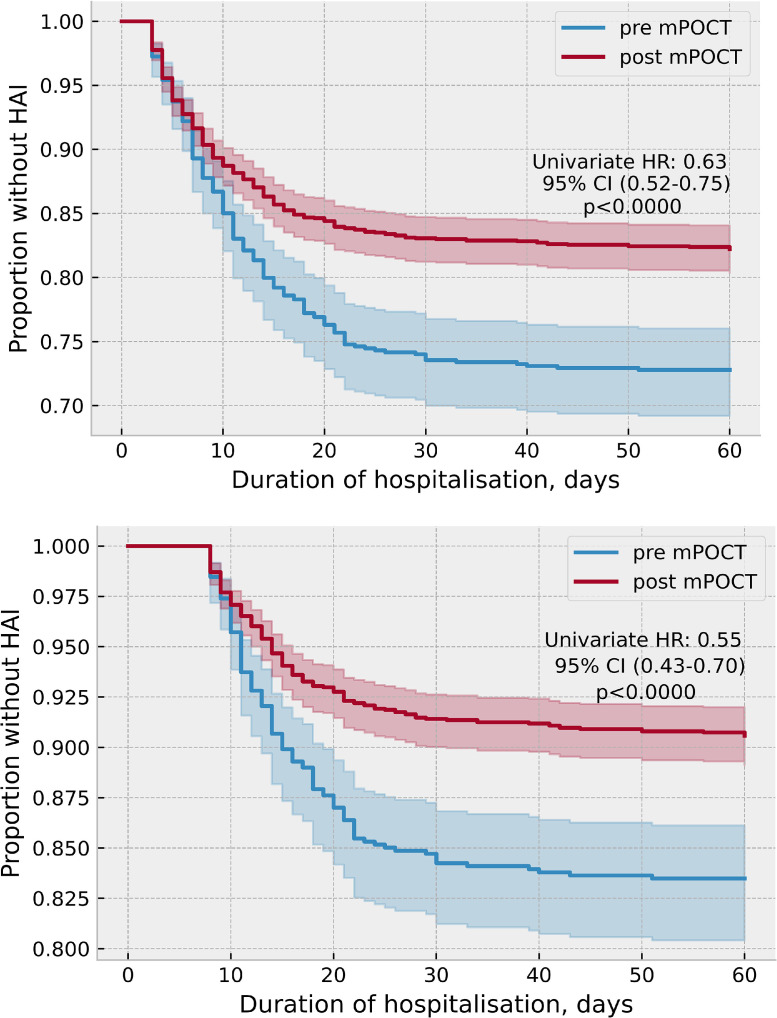
In this pre and post implementation study patients were evaluated across two time periods: March 1st to August 13th 2020, prior to the introduction of mPOCT in medical admissions areas, and 14th August 2020 to 1st April 2021, after mPOCT introduction. The primary outcome was proportion of HA-COVID-19 infection among all COVID-19 positive patients. Secondary outcome measures included time to SARS-CoV-2 results, length of time spent in the medical assessment area and comparison of local, regional and national proportions of HA-COVID-19.
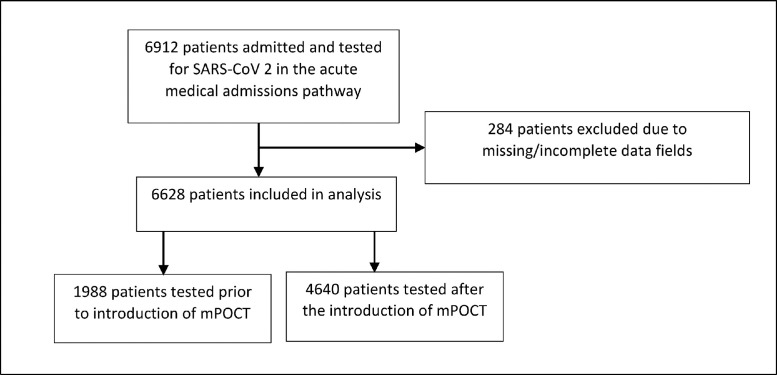
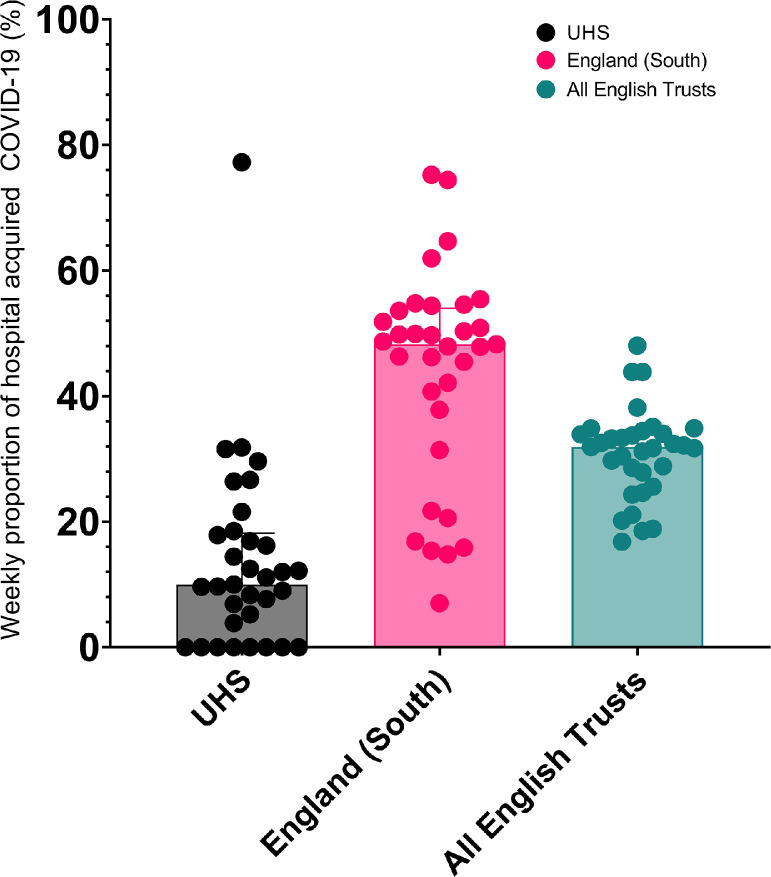
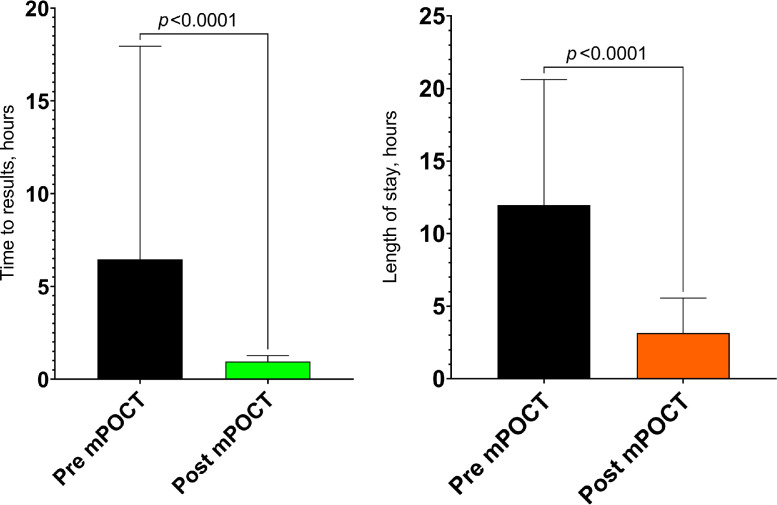
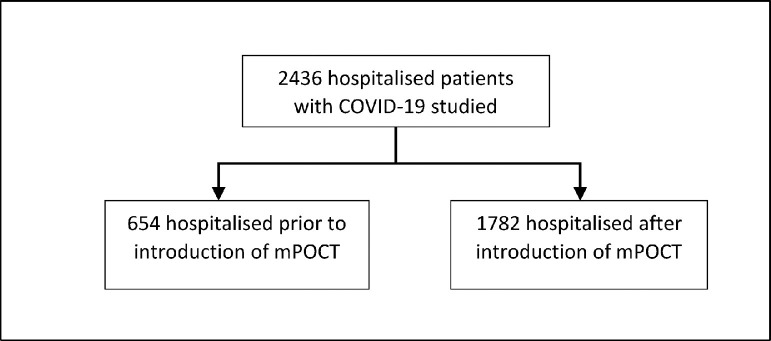
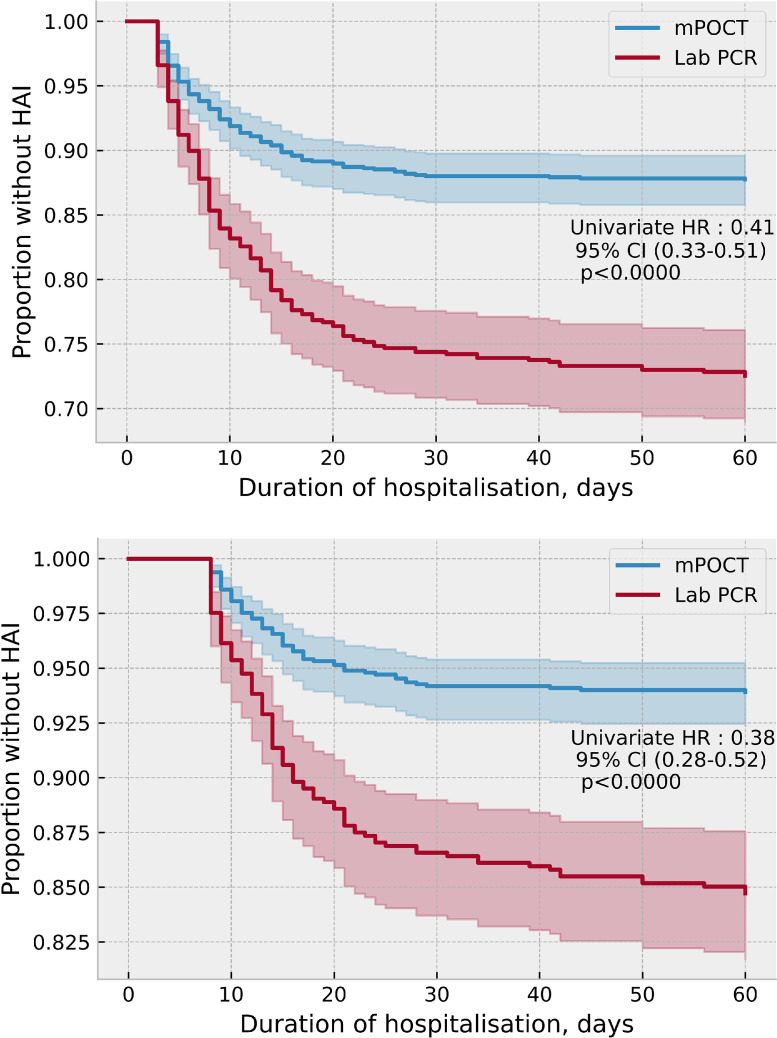
1988 patients were admitted through the acute medicine admission cohorting area and tested for SARS-CoV-2 prior to introducing mPOCT and 4640 afterwards. Median (IQR) time to SARS-CoV-2 result was 6.5 (2.1-17.9) hours prior to introducing mPOCT and 1.0 (0.8-1.3) hours afterwards (p < 0.0001). Median (IQR) duration in the assessment cohort area was 12.0 (4.8-20.6) hours prior to introduction of POCT and 3.2 (2.0-5.6) hours afterwards (p < 0.0001). The proportion of hospital-acquired COVID-19 cases was 108 (16.5%) of 654 prior to introducing mPOCT compared with 168 (9.4%) of 1782 afterwards, (HR 0.55, 95%CI 0.43-0.70; p < 0.0001). In the period following the introduction of mPOCT up to 1st April 2021 the median proportion of HA-COVID-19 was 13.6% (95%CI 8.2-18.9%) locally, compared with 43.8% (95%CI 37.8-49.9%) for all acute NHS trusts regionally and 30.9% (95%CI 28.4-33.5%) for all NHS trusts nationally.
Routine mPOCT for SARS-CoV-2 was associated with reduced time to results, time spent in admission cohort areas, and hospital-acquired COVID-19, compared to laboratory PCR.
将感染和未感染的患者集中在评估区域,同时等待实验室 PCR 结果,会增加医院获得性 COVID-19(HA-COVID-19)感染的风险。分子即时检测(mPOCT)可缩短结果报告时间并改善患者流程,但对 HA-COVID-19 的影响尚不清楚。
在这项实施前后的研究中,患者在两个时间段内进行评估:2020 年 3 月 1 日至 8 月 13 日,在医疗入院区引入 mPOCT 之前,以及 2020 年 8 月 14 日至 2021 年 4 月 1 日,在 mPOCT 引入之后。主要结局是所有 COVID-19 阳性患者中 HA-COVID-19 感染的比例。次要结局指标包括 SARS-CoV-2 结果的时间,在医疗评估区花费的时间以及比较当地,地区和全国 HA-COVID-19 的比例。
在引入 mPOCT 之前,有 1988 名患者通过急性医学入院区入院并接受了 SARS-CoV-2 检测,之后有 4640 名患者接受了检测。引入 mPOCT 之前,SARS-CoV-2 检测结果的中位数(IQR)为 6.5(2.1-17.9)小时,之后为 1.0(0.8-1.3)小时(p<0.0001)。引入 POCT 之前,评估队列区的中位数(IQR)时间为 12.0(4.8-20.6)小时,之后为 3.2(2.0-5.6)小时(p<0.0001)。在引入 mPOCT 之前,有 108 例(16.5%)的 654 例 COVID-19 患者发生医院获得性 COVID-19,而在引入 mPOCT 之后,有 1782 例中有 168 例(9.4%)发生医院获得性 COVID-19(HR 0.55,95%CI 0.43-0.70;p<0.0001)。在引入 mPOCT 后的时间段内,截至 2021 年 4 月 1 日,当地 HA-COVID-19 的中位数比例为 13.6%(95%CI 8.2-18.9%),而区域内所有急性 NHS 信托的中位数比例为 43.8%(95%CI 37.8-49.9%),全国所有 NHS 信托的中位数比例为 30.9%(95%CI 28.4-33.5%)。
与实验室 PCR 相比,SARS-CoV-2 的常规 mPOCT 与结果报告时间缩短,入院队列区花费的时间和医院获得性 COVID-19 减少有关。