Department of Medical Oncology, Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy.
Sorbonne Université, Department of Medical Oncology, Hôpital Saint-Antoine, AP-HP and INSERM, Unité Mixte de Recherche Scientifique 938, Centre de Recherche Saint-Antoine, Equipe Instabilité des Microsatellites et Cancer, Equipe labellisée par la Ligue Nationale contre le Cancer, Paris, France.
J Immunother Cancer. 2022 Feb;10(2). doi: 10.1136/jitc-2021-004001.
Despite unprecedented benefit from immune checkpoint inhibitors (ICIs) in patients with mismatch repair deficient (dMMR)/microsatellite instability high (MSI-H) advanced gastrointestinal cancers, a relevant proportion of patients shows primary resistance or short-term disease control. Since malignant effusions represent an immune-suppressed niche, we investigated whether peritoneal involvement with or without ascites is a poor prognostic factor in patients with dMMR/MSI-H metastatic colorectal cancer (mCRC) and gastric cancer (mGC) receiving ICIs.
We conducted a global multicohort study at Tertiary Cancer Centers and collected clinic-pathological data from a cohort of patients with dMMR/MSI-H mCRC treated with anti-PD-(L)1 ±anti-CTLA-4 agents at 12 institutions (developing set). A cohort of patients with dMMR/MSI-high mGC treated with anti-PD-1 agents±chemotherapy at five institutions was used as validating dataset.
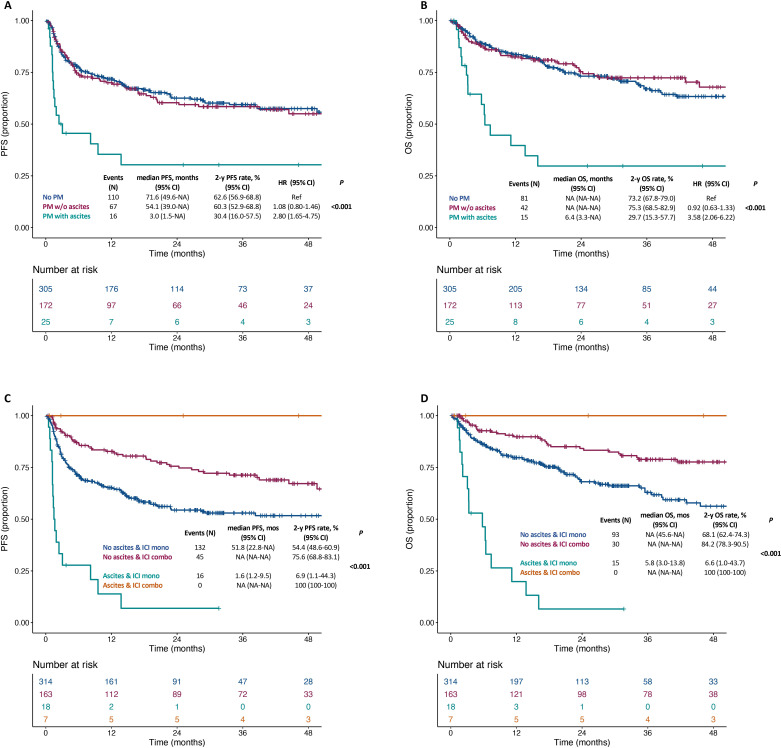
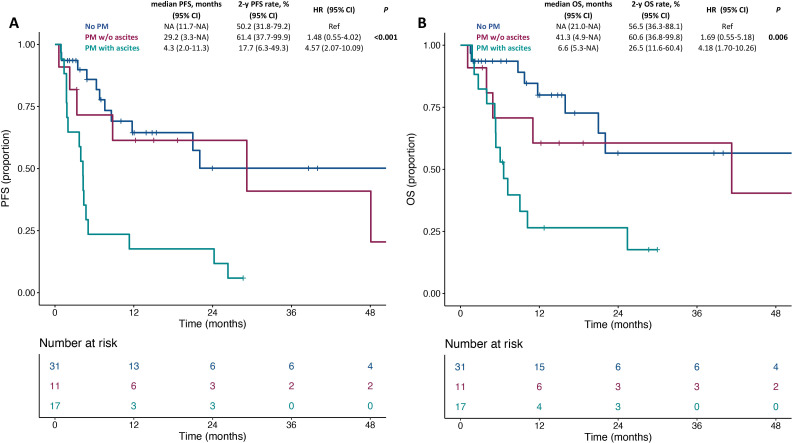
The mCRC cohort included 502 patients. After a median follow-up of 31.2 months, patients without peritoneal metastases and those with peritoneal metastases and no ascites had similar outcomes (adjusted HR (aHR) 1.15, 95% CI 0.85 to 1.56 for progression-free survival (PFS); aHR 0.96, 95% CI 0.65 to 1.42 for overall survival (OS)), whereas inferior outcomes were observed in patients with peritoneal metastases and ascites (aHR 2.90, 95% CI 1.70 to 4.94; aHR 3.33, 95% CI 1.88 to 5.91) compared with patients without peritoneal involvement. The mGC cohort included 59 patients. After a median follow-up of 17.4 months, inferior PFS and OS were reported in patients with peritoneal metastases and ascites (aHR 3.83, 95% CI 1.68 to 8.72; aHR 3.44, 95% CI 1.39 to 8.53, respectively), but not in patients with only peritoneal metastases (aHR 1.87, 95% CI 0.64 to 5.46; aHR 2.15, 95% CI 0.64 to 7.27) when compared with patients without peritoneal involvement.
Patients with dMMR/MSI-H gastrointestinal cancers with peritoneal metastases and ascites should be considered as a peculiar subgroup with highly unfavorable outcomes to current ICI-based therapies. Novel strategies to target the immune-suppressive niche in malignant effusions should be investigated, as well as next-generation ICIs or intraperitoneal approaches.
尽管免疫检查点抑制剂(ICIs)在错配修复缺陷(dMMR)/微卫星不稳定高(MSI-H)的晚期胃肠道癌症患者中带来了前所未有的获益,但仍有相当一部分患者表现出原发耐药或短期疾病控制。由于恶性积液代表了一个免疫抑制的生态位,我们研究了 dMMR/MSI-H 转移性结直肠癌(mCRC)和胃癌(mGC)患者是否存在腹膜受累(伴或不伴腹水)是预后不良的因素,这些患者接受了 ICI 治疗。
我们在三级癌症中心进行了一项全球性多队列研究,并从 12 个机构的接受抗 PD-(L)1 ±抗 CTLA-4 药物治疗的 dMMR/MSI-H mCRC 患者队列中收集了临床病理数据(开发队列)。来自五个机构的接受抗 PD-1 药物联合化疗治疗的 dMMR/MSI-high mGC 患者队列被用作验证数据集。
mCRC 队列纳入了 502 名患者。在中位随访 31.2 个月后,无腹膜转移的患者和仅有腹膜转移无腹水的患者的结局相似(无进展生存期的调整后 HR(aHR)为 1.15,95%CI 0.85 至 1.56;总生存期的 aHR 为 0.96,95%CI 0.65 至 1.42),而有腹膜转移和腹水的患者的结局则较差(aHR 为 2.90,95%CI 1.70 至 4.94;aHR 为 3.33,95%CI 1.88 至 5.91)。mGC 队列纳入了 59 名患者。在中位随访 17.4 个月后,有腹膜转移和腹水的患者的无进展生存期和总生存期更差(aHR 分别为 3.83,95%CI 1.68 至 8.72;aHR 分别为 3.44,95%CI 1.39 至 8.53),但仅有腹膜转移而无腹水的患者(aHR 为 1.87,95%CI 0.64 至 5.46;aHR 为 2.15,95%CI 0.64 至 7.27)与无腹膜受累的患者相比,其结局没有差异。
dMMR/MSI-H 胃肠道癌症患者如果存在腹膜转移和腹水,应被视为预后极差的特殊亚组,对目前基于 ICI 的治疗不敏感。应研究针对恶性积液中免疫抑制生态位的新策略,以及下一代 ICI 或腹腔内治疗方法。