a:1:{s:5:"en_US";s:47:"All India Institute of Medical Sciences Jodhpur";}.
Department of Pulmonary Medicine,All India Institute of Medical Sciences, Jodhpur.
Acta Biomed. 2021 Jul 1;92(3):e2021024. doi: 10.23750/abm.v92i3.10630.
The outbreak ofsevere acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic has resulted inexponential rise in the number of patients getting hospitalised with corona virus disease 2019 (COVID-19). There is a paucity of data from South East Asian Region related to the predictors of clinical outcomes in these patients. This formed the basis of conducting our study.
This was an analytical cross-sectional study. Demographic, clinical, radiological and laboratory data of 125 patients was collected on admission. The study outcome was death or discharge after recovery. For univariate analysis, unpaired t-test, Chi-square and Fisher's Exact test were used. Receiver operating characteristic (ROC) curves were plotted for Sequential Organ Failure Assessment (SOFA) score and few laboratory parameters. Logistic regression was applied for multivariate analysis.
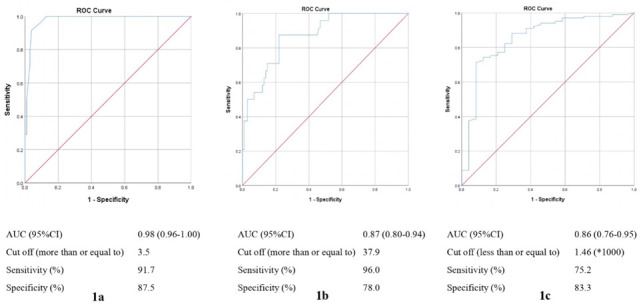
Elderly age, ischemic heart disease and smoking were significantly associated with mortality. Elevated levels of D-dimer and lactate dehydrogenase (LDH) and reduced lymphocyte counts were the predictors of mortality. The ROCs for SOFA score curve showed a cut-off value ≥ 3.5 (sensitivity- 91.7% and specificity- 87.5%), for IL-6 the cut-off value was ≥ 37.9 (sensitivity- 96% and specificity- 78%) and for lymphocyte counts, a cut off was calculated to be less than and equal to 1.46 x 109per litre (sensitivity-75.2%and specificity- 83.3%).
Old age, smoking history, ischemic heart disease and laboratory parameters including elevated D-dimer, raised LDH and low lymphocyte counts at baseline are associated with COVID-19 mortality. A higher SOFA score at admission is a poor prognosticator in COVID-19 patients.
严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)大流行的爆发导致因 2019 年冠状病毒病(COVID-19)住院的患者数量呈指数级增长。来自东南亚地区的关于这些患者临床结局预测因素的数据很少。这就是我们进行这项研究的基础。
这是一项分析性横断面研究。在入院时收集了 125 名患者的人口统计学、临床、影像学和实验室数据。研究结果是死亡或康复后出院。对于单变量分析,使用了配对 t 检验、卡方检验和 Fisher 精确检验。为序贯器官衰竭评估(SOFA)评分和一些实验室参数绘制了受试者工作特征(ROC)曲线。应用逻辑回归进行多变量分析。
年龄较大、缺血性心脏病和吸烟与死亡率显著相关。D-二聚体和乳酸脱氢酶(LDH)升高以及淋巴细胞计数减少是死亡的预测因素。SOFA 评分曲线的 ROC 显示截断值≥3.5(敏感性为 91.7%,特异性为 87.5%),IL-6 的截断值为≥37.9(敏感性为 96%,特异性为 78%),淋巴细胞计数的截断值计算为小于或等于 1.46 x 109/升(敏感性为 75.2%,特异性为 83.3%)。
年龄较大、吸烟史、缺血性心脏病和实验室参数,包括基线时 D-二聚体升高、LDH 升高和淋巴细胞计数降低,与 COVID-19 死亡率相关。入院时较高的 SOFA 评分是 COVID-19 患者预后不良的预测指标。