Willoughby James E, Baker Joseph F
School of Medicine, University of Auckland, Auckland, New Zealand.
Department of Surgery, University of Auckland, Auckland, New Zealand.
Global Spine J. 2023 Oct;13(8):2168-2175. doi: 10.1177/21925682221074659. Epub 2022 Feb 7.
Retrospective cohort study.
To validate the predictive accuracy of both the SpineSage and ACS-NSQIP surgical risk calculators in patients over the age of 80 years, undergoing spine surgery for any reason.
We included 210 consecutive patients treated with single-stage spine surgery at our institution between 2009 and 2019. The demographic details and preoperative characteristics of each patient were collected and reviewed for entry into both the SpineSage and ACS risk calculators. The estimated risk supplied by these calculators was compared to the observed rate of complications post-surgery. The main method of comparison was using receiver operating characteristic (ROC) curve analysis.
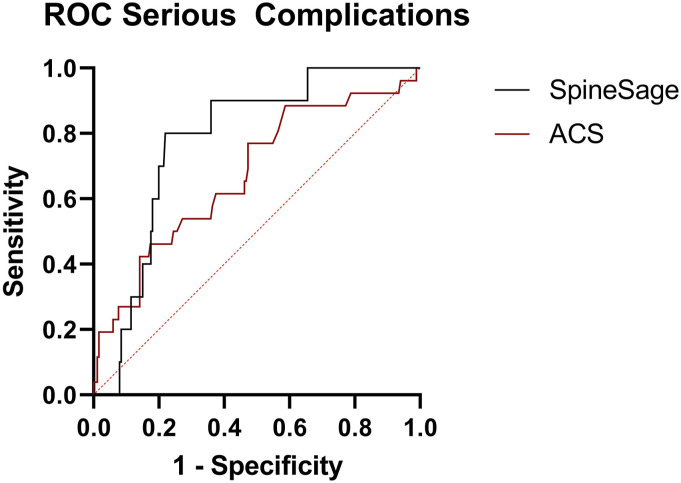
Complications were identified in 51 patients (24%). Most patients underwent surgery for a degenerative cause (71%), with the majority of procedures performed on the lumbosacral spine (66%). Receiver operating characteristic (ROC) curves were calculated to compare the outcomes of each tool. Area under the curve (AUC) analysis showed similar predictive accuracy between SpineSage and ACS when predicting overall complications (0.688; < .001 vs 0.634; = .021). AUC analysis demonstrated that SpineSage had better predictive accuracy when estimating risk of major complications (0.778; = .037 vs 0.675; = .001).
For the prediction of risks associated with spine surgery in those aged >80 years, SpineSage appears to be preferable to the ACS-NSQIP surgical risk calculator in this single centre cohort, SpineSage was more accurate in predicting the risk of serious medical complications. The accuracy of both of these tools could still be improved upon.
回顾性队列研究。
验证SpineSage和美国外科医师学会国家外科质量改进计划(ACS-NSQIP)手术风险计算器在80岁以上因任何原因接受脊柱手术患者中的预测准确性。
我们纳入了2009年至2019年期间在我们机构接受单阶段脊柱手术的210例连续患者。收集并审查了每位患者的人口统计学细节和术前特征,以输入SpineSage和ACS风险计算器。将这些计算器提供的估计风险与术后观察到的并发症发生率进行比较。主要的比较方法是使用受试者工作特征(ROC)曲线分析。
51例患者(24%)出现并发症。大多数患者因退行性病因接受手术(71%),大多数手术在腰骶部脊柱进行(66%)。计算受试者工作特征(ROC)曲线以比较每种工具的结果。曲线下面积(AUC)分析显示,在预测总体并发症时,SpineSage和ACS之间的预测准确性相似(0.688;P <.001 vs 0.634;P =.021)。AUC分析表明,在估计主要并发症风险时,SpineSage具有更好的预测准确性(0.778;P =.037 vs 0.675;P =.001)。
对于预测80岁以上患者脊柱手术相关风险,在这个单中心队列中,SpineSage似乎比ACS-NSQIP手术风险计算器更可取,SpineSage在预测严重医疗并发症风险方面更准确。这两种工具的准确性仍有提升空间。