Pakoz Zehra Betul, Ustaoglu Muge, Vatansever Sezgin, Yuksel Elif Saritas, Topal Firdevs
Katip Celebi University School of Medicine, Department of Gastroenterology, Izmir, Turkey.
Ondokuz Mayıs University School of Medicine, Department of Gastroenterology, Izmir, Turkey.
Gastroenterol Res Pract. 2022 Jan 31;2022:9987214. doi: 10.1155/2022/9987214. eCollection 2022.
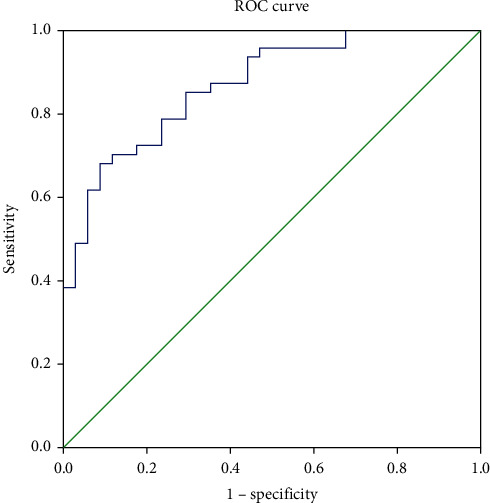
Radiologic and endoscopic diagnostic methods are used to determine disease activity in ulcerative colitis (UC). In order for endoscopic procedures to be invasive and to prevent radiation exposure, especially in young people, studies have been carried out frequently to determine a simple, fast, and reliable activity marker with laboratory methods. Our aim in this study is to determine the usefulness of serum immune-inflammatory index as a noninvasive marker of activation in patients with ulcerative colitis. A total of 82 consecutive patients treated with a diagnosis of ulcerative colitis were included in the study. The disease activation was assessed using the Mayo endoscopic subscore. The site of involvement was grouped into two as left colitis and extensive colitis. Patients were divided into two groups as those who had active disease based on clinical and endoscopic findings and those who were in remission. C-reactive protein (CRP) levels, platelets, neutrophils, and lymphocytes were recorded in all participants. The systemic immune-inflammation index (SII) and CRP values were compared between UC patients with active disease or remission. The correlations between CRP, SII, and Mayo endoscopic subscores were analyzed. In addition, ROC curve analysis for SII was performed to determine the cut-off value, sensitivity, and specificity in determining ulcerative colitis activity. The value of SII was significantly higher in the active group than the remission group (respectively, 1497 ± 1300 and 495 ± 224, < 0.001). In the correlation analysis, a significant correlation was found between SII and Mayo subscore. In ROC curve analysis, SII was found to be significantly effective in determining activity in ulcerative colitis patients. For 0.860 area under the curve, the sensitivity was 68.1% and the specificity was 91.2% at a cut-off value of 781.5. SII is significantly higher in patients with active ulcerative colitis than those in remission. It shows promise for use as a noninvasive marker of active ulcerative colitis.
放射学和内镜诊断方法用于确定溃疡性结肠炎(UC)的疾病活动度。为了避免内镜检查具有侵入性以及防止辐射暴露,尤其是在年轻人中,人们频繁开展研究以通过实验室方法确定一种简单、快速且可靠的活动标志物。本研究的目的是确定血清免疫炎症指数作为溃疡性结肠炎患者激活状态的非侵入性标志物的有用性。本研究纳入了总共82例连续诊断为溃疡性结肠炎并接受治疗的患者。使用梅奥内镜子评分评估疾病激活情况。受累部位分为左半结肠炎和广泛性结肠炎两组。根据临床和内镜检查结果,将患者分为疾病活动组和缓解组。记录所有参与者的C反应蛋白(CRP)水平、血小板、中性粒细胞和淋巴细胞。比较活动期或缓解期UC患者的全身免疫炎症指数(SII)和CRP值。分析CRP、SII与梅奥内镜子评分之间的相关性。此外,对SII进行ROC曲线分析以确定在判断溃疡性结肠炎活动度时的临界值、敏感性和特异性。活动组的SII值显著高于缓解组(分别为1497±1300和495±224,<0.001)。在相关性分析中,发现SII与梅奥子评分之间存在显著相关性。在ROC曲线分析中,发现SII在判断溃疡性结肠炎患者的活动度方面显著有效。曲线下面积为0.860时,在临界值为781.5时,敏感性为68.1%,特异性为91.2%。活动期溃疡性结肠炎患者的SII显著高于缓解期患者。它有望用作活动期溃疡性结肠炎的非侵入性标志物。