Department of Breast Surgery, Fujian Medical University Union Hospital, Fuzhou, Fujian, Fujian Province, China.
Department of General Surgery, Fujian Medical University Union Hospital, Fuzhou, Fujian, Fujian Province, China.
JAMA Netw Open. 2022 Feb 1;5(2):e2145934. doi: 10.1001/jamanetworkopen.2021.45934.
Studies have shown that delayed initiation of surgery and adjuvant chemotherapy is associated with lower rates of breast cancer survival. However, it remains unclear whether delayed initiation of adjuvant hormone therapy (AHT) is associated with survival.
To assess the association of time to adjuvant hormone therapy (TTH) with breast cancer survival and evaluate the factors associated with AHT.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study examined data from the National Cancer Database from 2004 through 2014 to assess the association of TTH (stratified as ≤150 and >150 days) with cancer survival. All patients included were diagnosed with stage I to stage III hormone receptor-positive, human epidermal growth factor receptor-2 (ERBB2; formerly HER2)-negative invasive breast cancer and underwent AHT without chemotherapy. Data were analyzed from April 2019 to May 2020.
AHT was administered at different time points following surgical procedures for breast cancer treatment.
An inverse probability of treatment weighting (IPTW) model was constructed to evaluate overall survival by adjusting for treatment facility, patient demographics, tumor characteristics, and treatment; multivariable logistic regression was conducted to assess factors associated with delayed treatment.
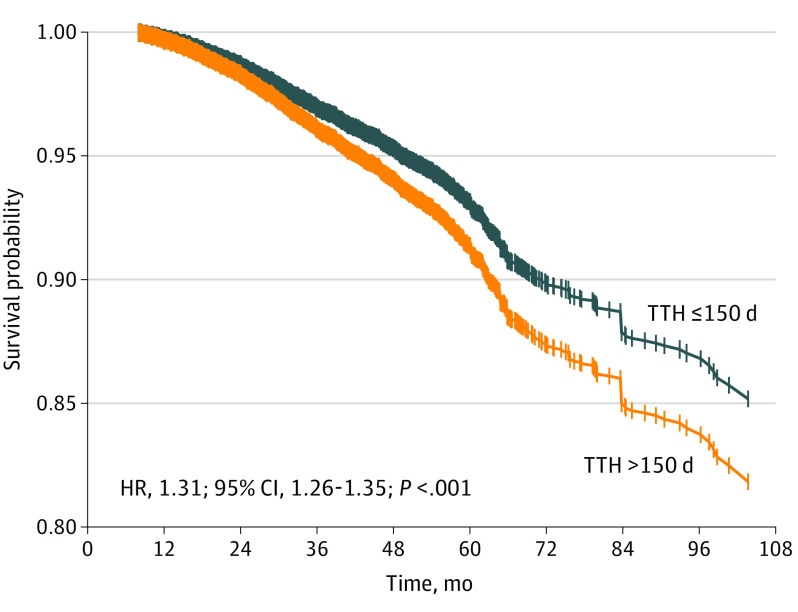
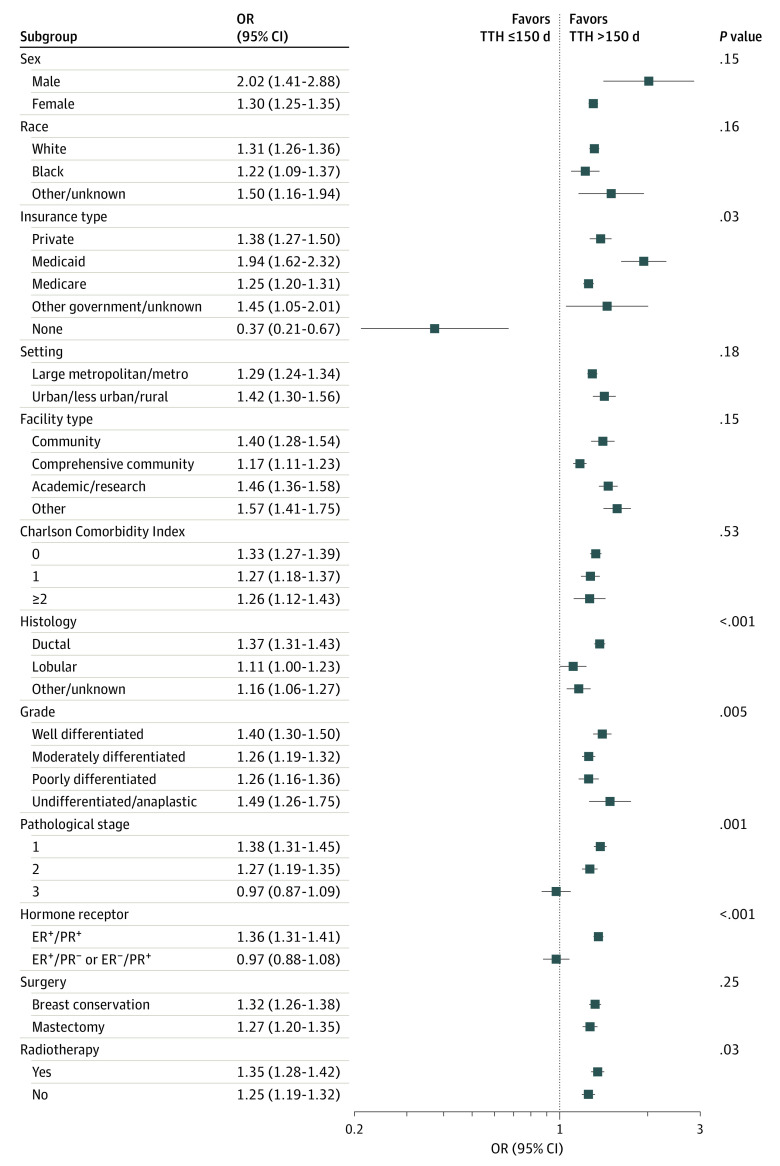
A total of 144 103 patients (median [IQR] follow-up, 36.6 months [25.5-49.2 months]; mean [SD] age, 63.7 [11.6] years) were identified, which included 142 916 (99.2%) women, 11 574 (8.0%) Black patients, and 126 013 (87.4%) White patients. Of these, 134 873 patients (93.6%) had a TTH of 150 days or less and 9230 patients (6.4%) had a TTH longer than 150 days. The IPTW-based Cox model demonstrated that patients with delayed AHT (ie, a TTH past 150 days) were associated with decreased survival (hazard ratio [HR], 1.31; 95% CI, 1.26-1.35; P < .001) compared with those receiving the timely treatment (TTH ≤150 days). Several sensitivity analyses (including IPTW with stabilized weight [HR, 1.31; 95% CI, 1.19-1.45; P < .001], propensity score matching [HR, 1.41; 1.13-1.76; P = .002], and propensity score regression adjustment [HR, 1.29; 95% CI, 1.16-1.43; P < .001]) and exploratory subgroup analyses yielded similar trends. Factors associated with delayed AHT included Black racial identity (OR, 1.66; 95% CI, 1.55-1.77), nonprivate insurance (eg, no insurance: OR, 1.46; 95% CI, 1.26-1.70), living in large metropolitan or metropolitan areas (reference vs urban, less urban, or rural: OR, 0.82; 95% CI, 0.76-0.87), treatment in a community hospital (reference vs academic or research: OR, 0.91; 95% CI, 0.84-0.98), Charlson-Deyo Comorbidity Index score 2 or higher (OR, 1.17; 95% CI, 1.04-1.32), poor grade differentiation (OR, 1.42; 95% CI, 1.32-1.53), II and III pathological stage (stage III: OR, 3.13; 95% CI, 2.76-3.54), estrogen receptor-positive (ER+)/progesterone receptor-negative (PR-) or ER-/PR+ (OR, 1.22; 95% CI, 1.13-1.31), receiving breast conservation surgery (reference vs mastectomy: OR, 0.87; 95% CI, 0.79-0.94), and radiotherapy (reference vs no radiotherapy: OR, 0.56; 95% CI, 0.52-0.61).
The delay of the initiation of AHT past 150 days was associated with diminished survival in hormone receptor-positive, ERBB2-negative patients with breast cancer who did not receive chemotherapy. Efforts should be made to address factors associated with delayed treatment to improve survival.
研究表明,手术和辅助化疗的延迟启动与乳腺癌生存率降低有关。然而,辅助激素治疗(AHT)的延迟启动是否与生存有关仍不清楚。
评估辅助激素治疗时间(TTH)与乳腺癌生存的关系,并评估与 AHT 相关的因素。
设计、地点和参与者:这项队列研究利用 2004 年至 2014 年期间国家癌症数据库的数据,评估 TTH(分层为≤150 天和>150 天)与癌症生存的关系。所有纳入的患者均被诊断为 I 期至 III 期激素受体阳性、人表皮生长因子受体 2(ERBB2;以前称为 HER2)阴性浸润性乳腺癌,并在未接受化疗的情况下接受 AHT。数据分析于 2019 年 4 月至 2020 年 5 月进行。
AHT 在乳腺癌治疗后的不同时间点进行。
构建逆概率治疗加权(IPTW)模型,通过调整治疗机构、患者人口统计学特征、肿瘤特征和治疗来评估总生存率;进行多变量逻辑回归分析,以评估与延迟治疗相关的因素。
共纳入 144103 例患者(中位[IQR]随访时间,36.6 个月[25.5-49.2 个月];平均[SD]年龄,63.7[11.6]岁),其中 142916 例(99.2%)为女性,11574 例(8.0%)为黑人患者,126013 例(87.4%)为白人患者。其中,134873 例(93.6%)的 TTH 为 150 天或更短,9230 例(6.4%)的 TTH 长于 150 天。基于 IPTW 的 Cox 模型表明,与接受及时治疗(TTH≤150 天)的患者相比,接受延迟 AHT(即 TTH 超过 150 天)的患者生存率降低(风险比[HR],1.31;95%CI,1.26-1.35;P<0.001)。几项敏感性分析(包括使用稳定权重的 IPTW[HR,1.31;95%CI,1.19-1.45;P<0.001]、倾向评分匹配[HR,1.41;95%CI,1.13-1.76;P=0.002]和倾向评分回归调整[HR,1.29;95%CI,1.16-1.43;P<0.001])和探索性亚组分析得出了类似的趋势。与延迟 AHT 相关的因素包括黑人种族身份(OR,1.66;95%CI,1.55-1.77)、非私人保险(例如,无保险:OR,1.46;95%CI,1.26-1.70)、居住在大都市或大都市区(参考城市、欠城市或农村:OR,0.82;95%CI,0.76-0.87)、在社区医院接受治疗(参考学术或研究机构:OR,0.91;95%CI,0.84-0.98)、Charlson-Deyo 合并症指数评分 2 或更高(OR,1.17;95%CI,1.04-1.32)、分化不良(OR,1.42;95%CI,1.32-1.53)、II 期和 III 期病理阶段(III 期:OR,3.13;95%CI,2.76-3.54)、雌激素受体阳性(ER+)/孕激素受体阴性(PR-)或 ER-/PR+(OR,1.22;95%CI,1.13-1.31)、接受保乳手术(参考乳房切除术:OR,0.87;95%CI,0.79-0.94)和放疗(参考无放疗:OR,0.56;95%CI,0.52-0.61)。
在未接受化疗的激素受体阳性、ERBB2 阴性乳腺癌患者中,AHT 启动时间延迟超过 150 天与生存率降低有关。应努力解决与延迟治疗相关的因素,以提高生存率。