Anderko Renee R, Gómez Hernando, Canna Scott W, Shakoory Bita, Angus Derek C, Yealy Donald M, Huang David T, Kellum John A, Carcillo Joseph A
Department of Critical Care Medicine, University of Pittsburgh, Pittsburgh, PA, USA.
Center for Critical Care Nephrology, Department of Critical Care Medicine, University of Pittsburgh, School of Medicine, 3550 Terrace Street, 6th floor Scaife Hall, Pittsburgh, PA, 15261, USA.
Intensive Care Med Exp. 2022 Feb 21;10(1):6. doi: 10.1186/s40635-022-00433-y.
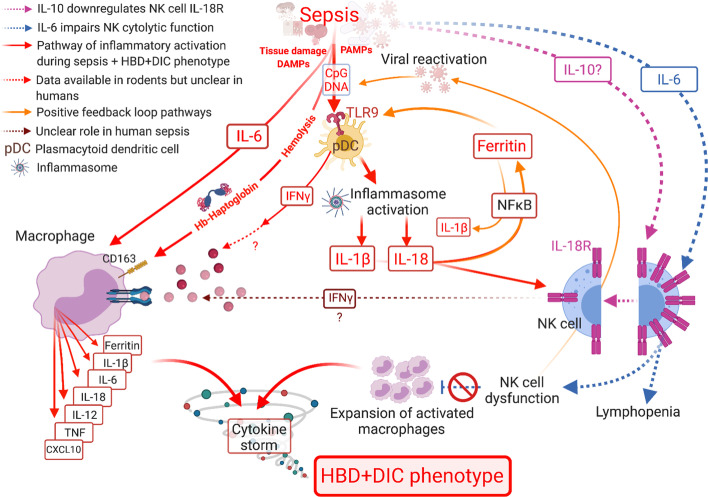
Interleukin-1 receptor antagonists can reduce mortality in septic shock patients with hepatobiliary dysfunction and disseminated intravascular coagulation (HBD + DIC), an organ failure pattern with inflammatory features consistent with macrophage activation. Identification of clinical phenotypes in sepsis may allow for improved care. We aim to describe the occurrence of HBD + DIC in a contemporary cohort of patients with sepsis and determine the association of this phenotype with known macrophage activation syndrome (MAS) biomarkers and mortality. We performed a retrospective nested case-control study in adult septic shock patients with concurrent HBD + DIC and an equal number of age-matched controls, with comparative analyses of all-cause mortality and circulating biomarkers between the groups. Multiple logistic regression explored the effect of HBD + DIC on mortality and the discriminatory power of the measured biomarkers for HBD + DIC and mortality.
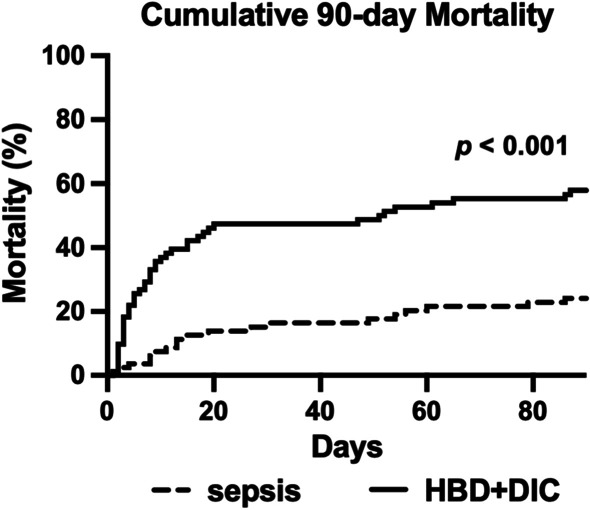
Six percent of septic shock patients (n = 82/1341) had HBD + DIC, which was an independent risk factor for 90-day mortality (OR = 3.1, 95% CI 1.4-7.5, p = 0.008). Relative to sepsis controls, the HBD + DIC cohort had increased levels of 21 of the 26 biomarkers related to macrophage activation (p < 0.05). This panel was predictive of both HBD + DIC (sensitivity = 82%, specificity = 84%) and mortality (sensitivity = 92%, specificity = 90%).
The HBD + DIC phenotype identified patients with high mortality and a molecular signature resembling that of MAS. These observations suggest trials of MAS-directed therapies are warranted.
白细胞介素-1受体拮抗剂可降低伴有肝胆功能障碍和弥散性血管内凝血(HBD + DIC)的脓毒性休克患者的死亡率,HBD + DIC是一种具有与巨噬细胞活化一致的炎症特征的器官衰竭模式。识别脓毒症的临床表型可能有助于改善治疗。我们旨在描述当代脓毒症患者队列中HBD + DIC的发生情况,并确定该表型与已知的巨噬细胞活化综合征(MAS)生物标志物及死亡率之间的关联。我们对成年脓毒性休克患者进行了一项回顾性巢式病例对照研究,这些患者同时患有HBD + DIC,并设置了同等数量的年龄匹配对照,对两组间的全因死亡率和循环生物标志物进行了比较分析。多元逻辑回归探讨了HBD + DIC对死亡率的影响以及所测生物标志物对HBD + DIC和死亡率的判别能力。
6%的脓毒性休克患者(n = 82/1341)患有HBD + DIC,这是90天死亡率的独立危险因素(OR = 3.1,95%CI 1.4 - 7.5,p = 0.008)。相对于脓毒症对照组,HBD + DIC队列中与巨噬细胞活化相关的26种生物标志物中有21种水平升高(p < 0.05)。该生物标志物组合对HBD + DIC(敏感性 = 82%,特异性 = 84%)和死亡率(敏感性 = 92%,特异性 = 90%)均具有预测作用。
HBD + DIC表型识别出了死亡率高且分子特征类似于MAS的患者。这些观察结果表明有必要进行针对MAS的治疗试验。