Brain Mapping Unit, Department of Psychiatry, University of Cambridge, Cambridge, UK.
The Alan Turing Institute, British Library, London, UK.
Sci Rep. 2022 Feb 23;12(1):3039. doi: 10.1038/s41598-022-06766-8.
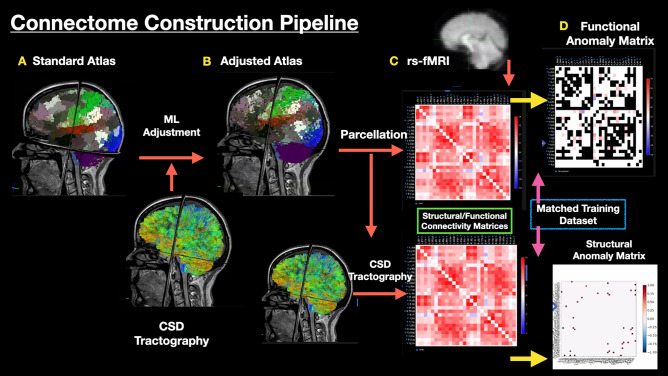
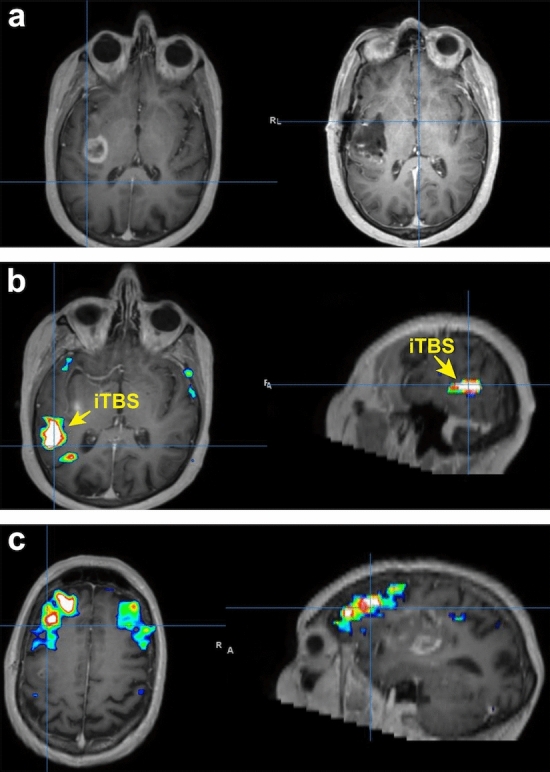
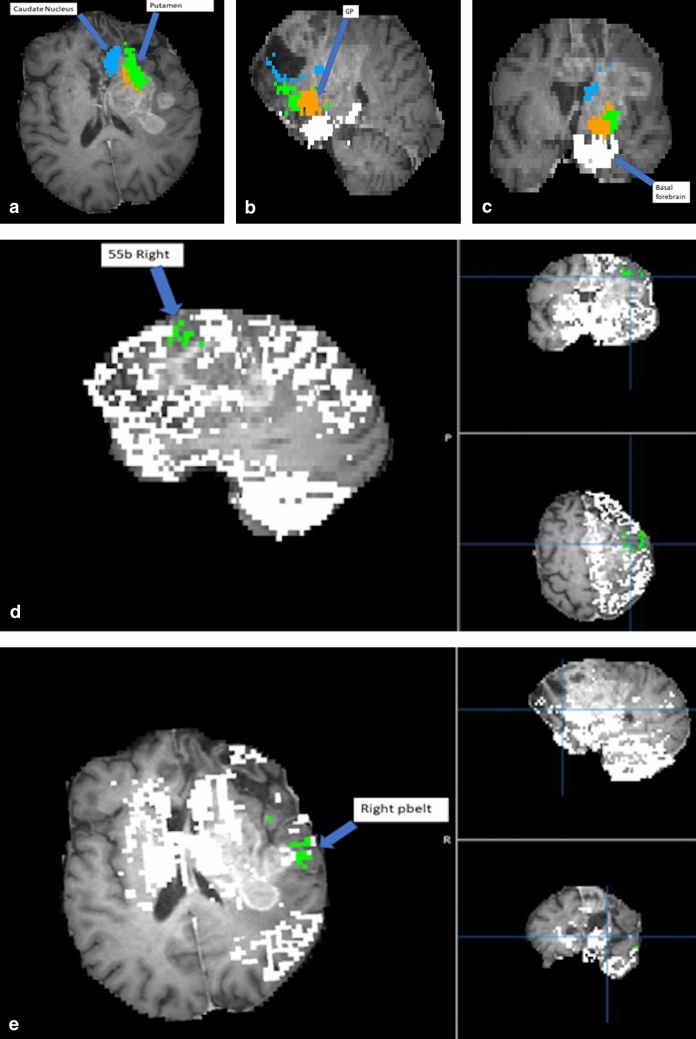
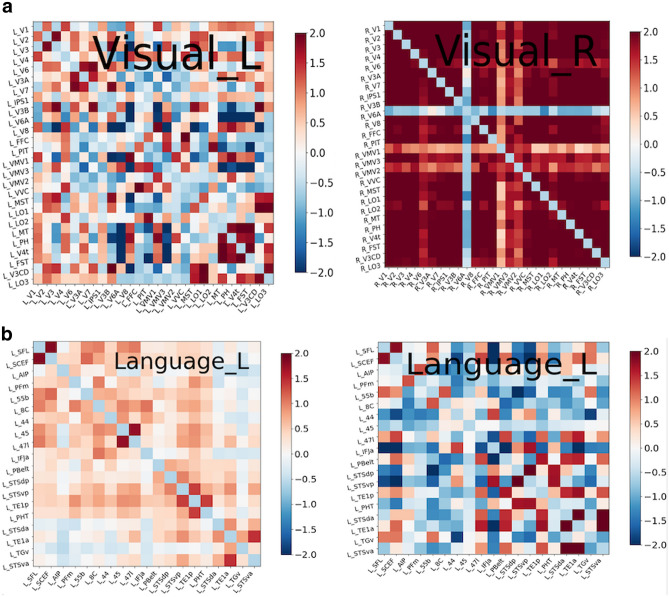
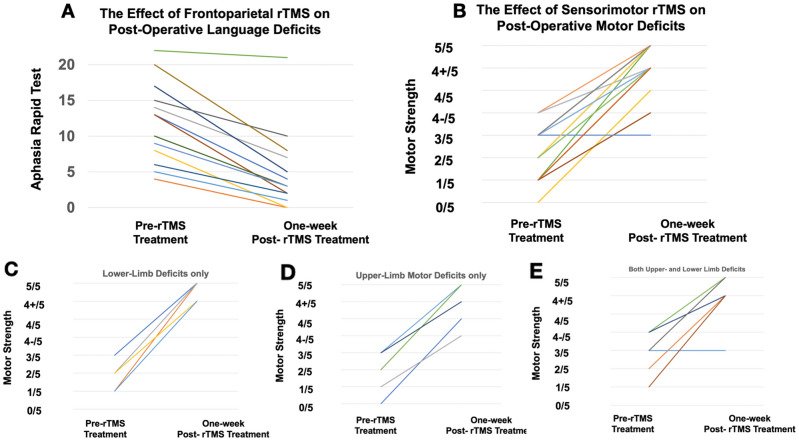
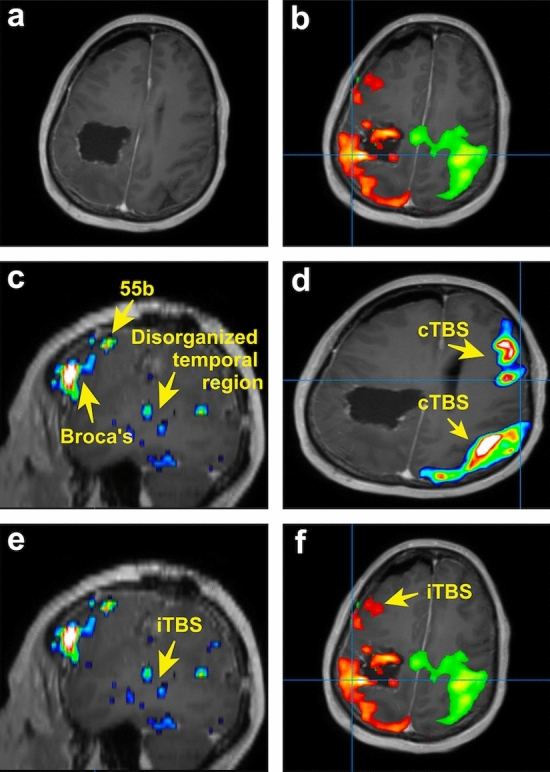
The human brain is a highly plastic 'complex' network-it is highly resilient to damage and capable of self-reorganisation after a large perturbation. Clinically, neurological deficits secondary to iatrogenic injury have very few active treatments. New imaging and stimulation technologies, though, offer promising therapeutic avenues to accelerate post-operative recovery trajectories. In this study, we sought to establish the safety profile for 'interventional neurorehabilitation': connectome-based therapeutic brain stimulation to drive cortical reorganisation and promote functional recovery post-craniotomy. In n = 34 glioma patients who experienced post-operative motor or language deficits, we used connectomics to construct single-subject cortical networks. Based on their clinical and connectivity deficit, patients underwent network-specific transcranial magnetic stimulation (TMS) sessions daily over five consecutive days. Patients were then assessed for TMS-related side effects and improvements. 31/34 (91%) patients were successfully recruited and enrolled for TMS treatment within two weeks of glioma surgery. No seizures or serious complications occurred during TMS rehabilitation and 1-week post-stimulation. Transient headaches were reported in 4/31 patients but improved after a single session. No neurological worsening was observed while a clinically and statistically significant benefit was noted in 28/31 patients post-TMS. We present two clinical vignettes and a video demonstration of interventional neurorehabilitation. For the first time, we demonstrate the safety profile and ability to recruit, enroll, and complete TMS acutely post-craniotomy in a high seizure risk population. Given the lack of randomisation and controls in this study, prospective randomised sham-controlled stimulation trials are now warranted to establish the efficacy of interventional neurorehabilitation following craniotomy.
人类大脑是一个高度灵活的“复杂”网络,它对损伤具有很强的弹性,并且在受到大的干扰后能够自我重组。临床上,由于医源性损伤导致的神经功能缺损几乎没有有效的治疗方法。然而,新的成像和刺激技术为加速术后恢复轨迹提供了有前途的治疗途径。在这项研究中,我们试图确定“介入性神经康复”的安全性:基于连接组学的治疗性脑刺激以驱动皮质重组并促进开颅术后的功能恢复。在 34 名经历术后运动或语言功能缺损的胶质瘤患者中,我们使用连接组学构建了单个患者的皮质网络。根据他们的临床和连接缺损,患者在连续 5 天内每天接受针对网络的经颅磁刺激(TMS)治疗。然后评估患者 TMS 相关的副作用和改善情况。34 名患者中有 31 名(91%)成功招募并在胶质瘤手术后两周内接受 TMS 治疗。在 TMS 康复和刺激后 1 周内没有发生癫痫发作或严重并发症。4 名患者报告短暂头痛,但在单次治疗后有所改善。在接受 TMS 后,没有观察到神经功能恶化,而 28 名患者中有 28 名患者在临床和统计学上都有显著的改善。我们展示了两个临床病例和一个介入性神经康复的视频演示。我们首次证明了在高癫痫发作风险人群中,在开颅术后即刻招募、入组和完成 TMS 的安全性和能力。鉴于本研究缺乏随机分组和对照,现在需要进行前瞻性随机假刺激对照试验,以确定开颅术后介入性神经康复的疗效。