Mucosal Entry of HIV and Mucosal Immunity, Institut Cochin, Université de Paris, Paris, France.
Institut National de la Santé et de la Recherche Médicale (INSERM) U1016, Paris, France.
Front Immunol. 2022 Feb 11;12:781923. doi: 10.3389/fimmu.2021.781923. eCollection 2021.
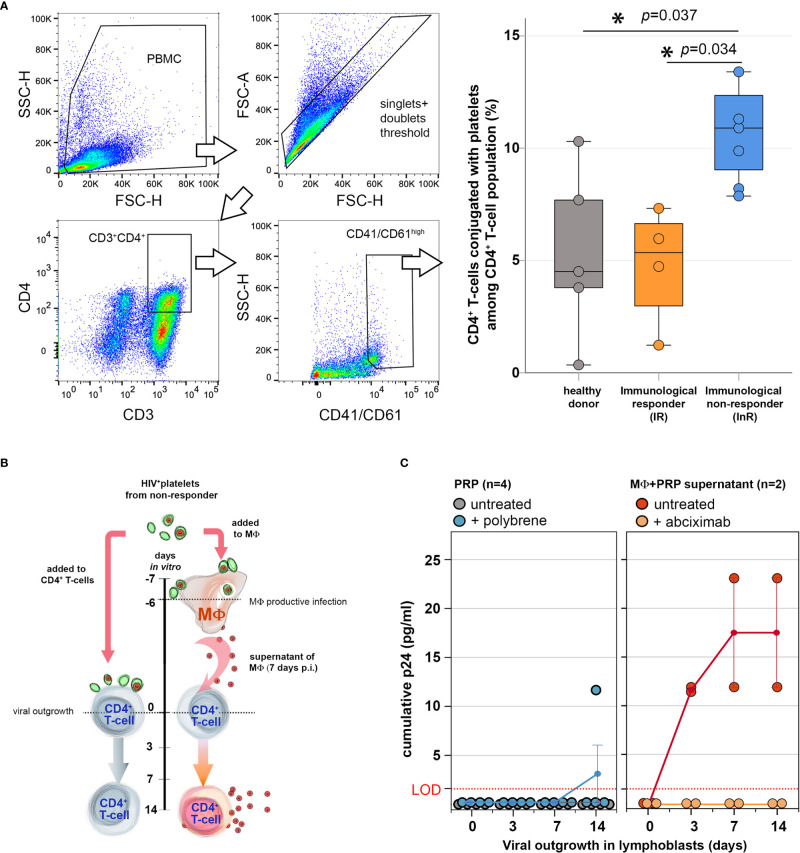
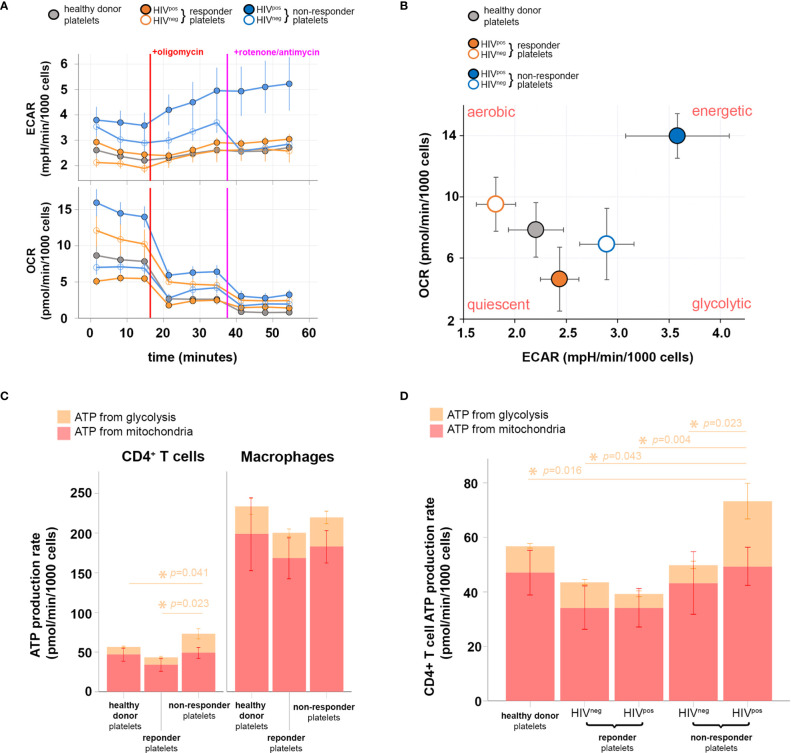
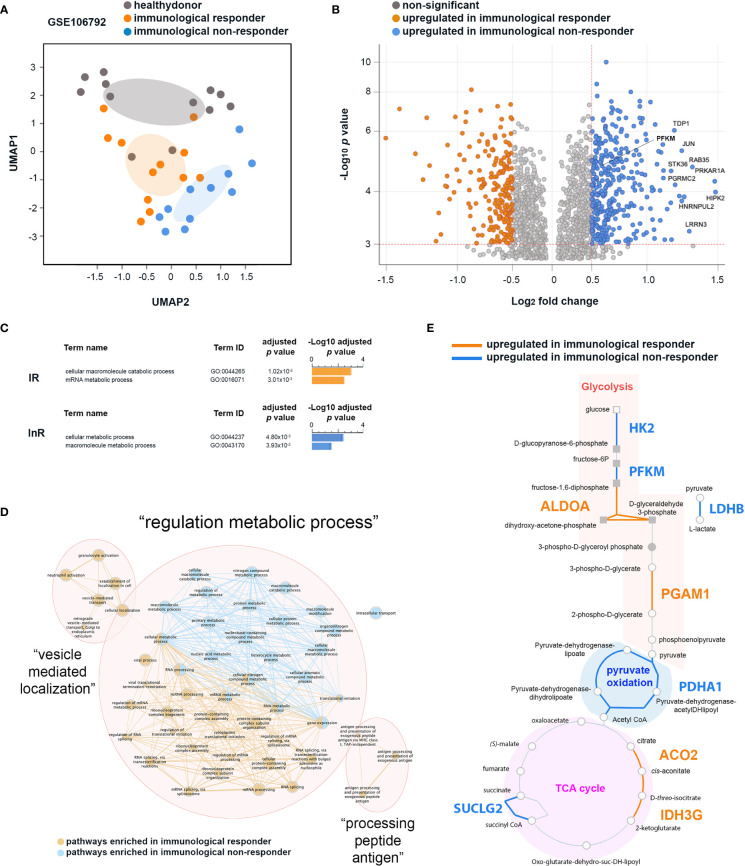
Immunological non-responders (InRs) are HIV-infected individuals in whom the administration of combination antiretroviral therapy (cART), although successful in suppressing viral replication, cannot properly reconstitute patient circulating CD4 T-cell number to immunocompetent levels. The causes for this immunological failure remain elusive, and no therapeutic strategy is available to restore a proper CD4 T-cell immune response in these individuals. We have recently demonstrated that platelets harboring infectious HIV are a hallmark of InR, and we now report on a causal connection between HIV-containing platelets and T-cell dysfunctions. We show here that , platelet-T-cell conjugates are more frequent among CD4 T cells in InRs displaying HIV-containing platelets (<350 CD4 T cells/μl blood for >1 year) as compared with healthy donors or immunological responders (IRs; >350 CD4 T cells/μl). This contact between platelet containing HIV and T cell in the conjugates is not infectious for CD4 T cells, as coculture of platelets from InRs containing HIV with healthy donor CD4 T cells fails to propagate infection to CD4 T cells. In contrast, when macrophages are the target of platelets containing HIV from InRs, macrophages become infected. Differential transcriptomic analyses comparing InR and IR CD4 T cells reveal an upregulation of genes involved in both aerobic and anaerobic glycolysis in CD4 T cells from InR vs. IR individuals. Accordingly, InR platelets containing HIV induce a dysfunctional increase in glycolysis-mediated energy production in CD4 T cells as compared with T cells cocultured with IR platelets devoid of virus. In contrast, macrophage metabolism is not affected by platelet contact. Altogether, this brief report demonstrates a direct causal link between presence of HIV in platelets and T-cell dysfunctions typical of InR, contributing to devise a platelet-targeted therapy for improving immune reconstitution in these individuals.
免疫无应答者(InRs)是感染 HIV 的个体,尽管联合抗逆转录病毒疗法(cART)成功抑制了病毒复制,但不能将患者循环 CD4 T 细胞数量适当重建到免疫功能正常的水平。这种免疫失败的原因仍然难以捉摸,目前尚无治疗策略可用于恢复这些个体的适当 CD4 T 细胞免疫反应。我们最近证明,携带感染性 HIV 的血小板是 InR 的一个标志,现在我们报告了 HIV 感染血小板与 T 细胞功能障碍之间的因果关系。我们在这里表明,与健康供体或免疫应答者(IRs;>350 CD4 T 细胞/μl)相比,在显示含有 HIV 的血小板的 InR 中,CD4 T 细胞中存在更多的血小板-T 细胞缀合物(血液中 CD4 T 细胞<350/μl 持续>1 年)。这种在缀合物中包含 HIV 的血小板与 T 细胞之间的接触对 CD4 T 细胞没有传染性,因为将来自包含 HIV 的 InR 的血小板与健康供体 CD4 T 细胞共培养不能将感染传播到 CD4 T 细胞。相比之下,当含有 HIV 的血小板的靶标是来自 InR 的巨噬细胞时,巨噬细胞会被感染。比较 InR 和 IR CD4 T 细胞的差异转录组分析显示,与 IR 个体相比,InR CD4 T 细胞中涉及有氧和无氧糖酵解的基因上调。相应地,与与不含病毒的 IR 血小板共培养的 T 细胞相比,来自包含 HIV 的 InR 血小板诱导的糖酵解介导的能量产生的功能失调增加。相比之下,血小板接触不会影响巨噬细胞代谢。总之,这份简短的报告证明了 HIV 在血小板中的存在与 InR 中典型的 T 细胞功能障碍之间存在直接因果关系,有助于设计针对血小板的治疗方法来改善这些个体的免疫重建。