Krynytska Inna, Marushchak Mariya, Birchenko Inna, Dovgalyuk Alina, Tokarskyy Oleksandr
Department of Functional and Laboratory Diagnostics, I. Horbachevsky Ternopil National Medical University, Ternopil, Ukraine.
Department of Medical Biochemistry, I. Horbachevsky Ternopil National Medical University, Ternopil, Ukraine.
Iran J Microbiol. 2021 Dec;13(6):737-747. doi: 10.18502/ijm.v13i6.8072.
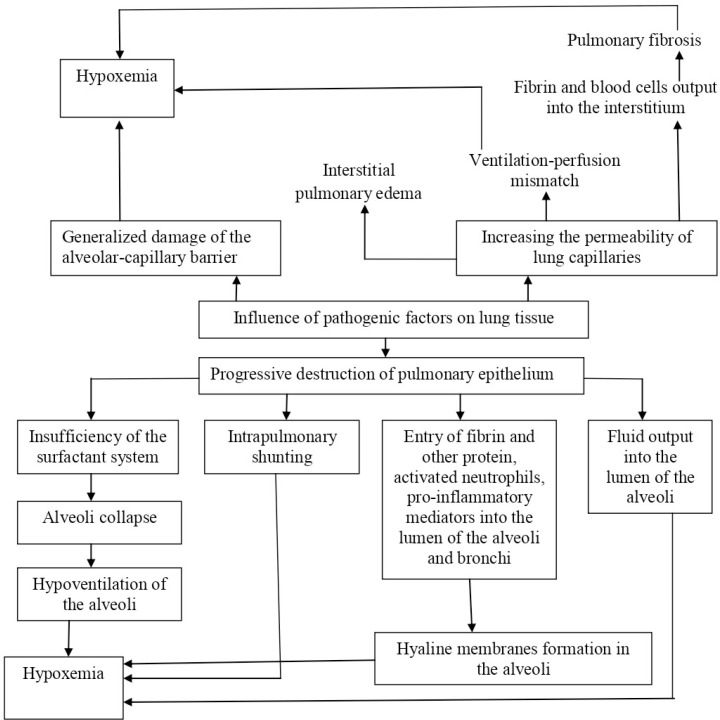
Coronavirus disease 2019 (COVID-19), caused by the novel coronavirus, Severe Acute Respiratory Syndrome-Coronavirus-2 (SARS-CoV-2), led to the ongoing global public health crisis. Existing clinical data suggest that COVID-19 patients with acute respiratory distress syndrome (ARDS) have worse outcomes and increased risk of intensive care unit (ICU) admission. The rapid increase in the numbers of patients requiring ICU care may imply a sudden and major challenge for affected health care systems. In this narrative review, we aim to summarize current knowledge of pathophysiology, clinical and morphological characteristics of COVID-19-associated ARDS and ARDS caused by other factors (classical ARDS) as defined by Berlin criteria, and therefore to elucidate the differences, which can affect clinical management of COVID-19-associated ARDS. Fully understanding the characteristics of COVID-19-associated ARDS will help identify its early progression and tailor the treatment, leading to improved prognosis in severe cases and reduced mortality. The notable mechanisms of COVID-19-associated ARDS include severe pulmonary infiltration/edema and inflammation, leading to impaired alveolar homeostasis, alteration of pulmonary physiology resulting in pulmonary fibrosis, endothelial inflammation and vascular thrombosis. Despite some distinct differences between COVID-19-associated ARDS and classical ARDS as defined by Berlin criteria, general treatment principles, such as lung-protective ventilation and rehabilitation concepts should be applied whenever possible. At the same time, ventilatory settings for COVID-19-associated ARDS require to be adapted in individual cases, depending on respiratory mechanics, recruitability and presentation timing.
2019冠状病毒病(COVID-19)由新型冠状病毒严重急性呼吸综合征冠状病毒2(SARS-CoV-2)引起,导致了持续的全球公共卫生危机。现有临床数据表明,患有急性呼吸窘迫综合征(ARDS)的COVID-19患者预后较差,入住重症监护病房(ICU)的风险增加。需要ICU护理的患者数量迅速增加,这可能意味着受影响的医疗系统面临突然且重大的挑战。在这篇叙述性综述中,我们旨在总结COVID-19相关ARDS以及由其他因素引起的ARDS(柏林标准定义的经典ARDS)的病理生理学、临床和形态学特征的现有知识,从而阐明可能影响COVID-19相关ARDS临床管理的差异。充分了解COVID-19相关ARDS的特征将有助于识别其早期进展并调整治疗方案,从而改善重症病例的预后并降低死亡率。COVID-19相关ARDS的显著机制包括严重的肺部浸润/水肿和炎症,导致肺泡稳态受损、肺生理改变导致肺纤维化、内皮炎症和血管血栓形成。尽管COVID-19相关ARDS与柏林标准定义的经典ARDS之间存在一些明显差异,但应尽可能应用一般治疗原则,如肺保护性通气和康复理念。同时,COVID-19相关ARDS的通气设置需要根据个体情况进行调整,具体取决于呼吸力学、可复张性和表现时机。