Malcolm Fisher Department of Intensive Care, The Royal North Shore Hospital, St Leonards, NSW, 2065, Australia.
The University of New South Wales, Kensington, Sydney, NSW, Australia.
Trials. 2022 Mar 4;23(1):199. doi: 10.1186/s13063-022-06104-3.
Developments in the care of critically ill patients with severe burns have led to improved hospital survival, but long-term recovery may be impaired. The extent to which patient-centred outcomes are assessed and reported in studies in this population is unclear.
We conducted a systematic review to assess the outcomes reported in studies involving critically ill burns patients. Randomised controlled trials (RCTs) and cohort studies on the topics of fluid resuscitation, analgesia, haemodynamic monitoring, ventilation strategies, transfusion targets, enteral nutrition and timing of surgery were included. We assessed the outcomes reported and then classified these according to two suggested core outcome sets.
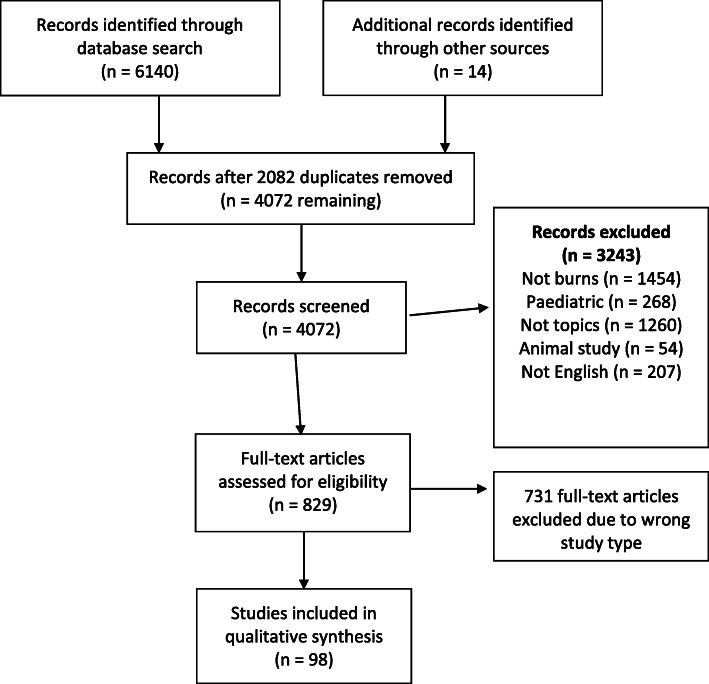
A comprehensive search returned 6154 studies; 98 papers met inclusion criteria. There were 66 RCTs, 19 clinical studies with concurrent controls and 13 interventional studies without concurrent controls. Outcome reporting was inconsistent across studies. Pain, reported using the visual analogue scale, fluid volume administered and mortality were the only outcomes measured in more than three studies. Sixty-six studies (67%) had surrogate primary outcomes. Follow-up was poor, with median longest follow-up across all studies 5 days (IQR 3-28). When compared to the suggested OMERACT core outcome set, 53% of papers reported on mortality, 28% reported on life impact, 30% reported resource/economic outcomes and 95% reported on pathophysiological manifestations. Burns-specific Falder outcome reporting was globally poor, with only 4.3% of outcomes being reported across the 98 papers.
There are deficiencies in the reporting of outcomes in the literature pertaining to the intensive care management of patients with severe burns, both with regard to the consistency of outcomes as well as a lack of focus on patient-centred outcomes. Long-term outcomes are infrequently reported. The development and validation of a core outcome dataset for severe burns would improve the quality of reporting.
危重病患者严重烧伤的治疗进展提高了住院生存率,但长期康复可能受损。目前尚不清楚在该人群的研究中,以患者为中心的结局评估和报告的程度如何。
我们进行了系统评价,以评估涉及危重病烧伤患者的研究中报告的结局。纳入了关于液体复苏、镇痛、血流动力学监测、通气策略、输血目标、肠内营养和手术时机的随机对照试验(RCT)和队列研究。我们评估了报告的结局,然后根据两个建议的核心结局集对这些结局进行分类。
全面检索共返回 6154 项研究;98 篇论文符合纳入标准。其中包括 66 项 RCT、19 项具有同期对照的临床研究和 13 项无同期对照的干预研究。研究之间的结局报告不一致。疼痛(使用视觉模拟评分法报告)、给予的液体量和死亡率是超过 3 项研究测量的唯一结局。66 项研究(67%)有替代主要结局。随访情况较差,所有研究中最长随访时间中位数为 5 天(IQR 3-28)。与建议的 OMERACT 核心结局集相比,53%的论文报告死亡率,28%报告生活影响,30%报告资源/经济结局,95%报告病理生理表现。烧伤特异性 Falder 结局报告总体较差,在 98 篇论文中仅报告了 4.3%的结局。
在严重烧伤患者的重症监护管理文献中,无论是在结局的一致性方面,还是在缺乏以患者为中心的结局方面,结局报告都存在缺陷。长期结局很少报告。严重烧伤核心结局数据集的制定和验证将提高报告质量。