Uehara Yuji, Hakozaki Taiki, Kitadai Rui, Narita Kosuke, Watanabe Kageaki, Hashimoto Kana, Kawai Shoko, Yomota Makiko, Hosomi Yukio
Department of Thoracic Oncology and Respiratory Medicine, Tokyo Metropolitan Cancer and Infectious Diseases Center, Komagome Hospital, Tokyo, Japan.
Transl Lung Cancer Res. 2022 Feb;11(2):135-149. doi: 10.21037/tlcr-21-815.
The baseline tumor size (BTS) is a prognostic factor for patients with non-small cell lung cancer (NSCLC) who received immune checkpoint inhibitor monotherapy (ICI-mono). However, this relationship is not yet known in patients treated with ICI in combination with chemotherapy (ICI-chemo).
This single-center retrospective study evaluated 159 patients with advanced NSCLC who received first-line ICI-mono or ICI-chemo from January 2016 to April 2021. Their BTS values were estimated using the maximum BTS (max BTS) (maximum target lesions' longest diameter) and total BTS (sum of target lesions' longest diameters) in a radiological assessment according to the Response Evaluation Criteria for Solid Tumors.
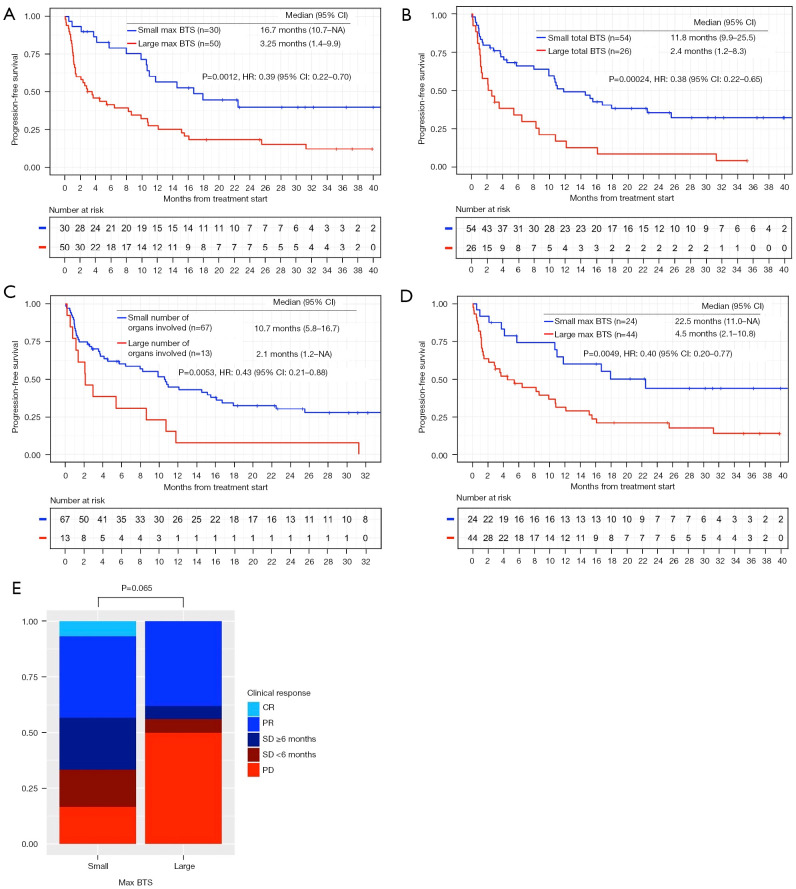
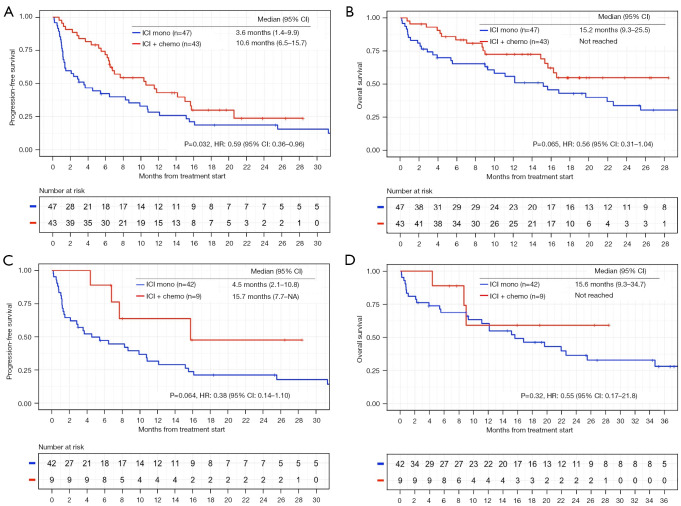
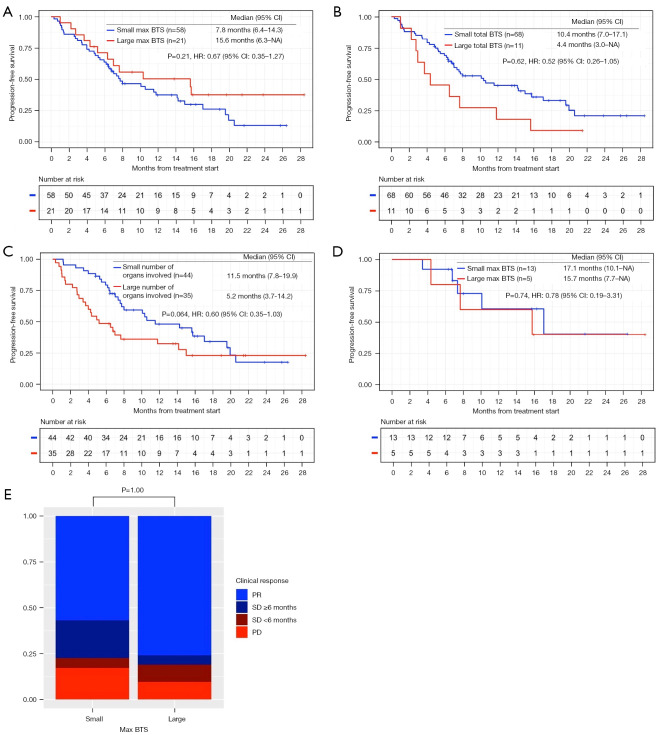
Based on a multivariable analysis, the large max BTS group had worse progression-free survival (PFS) in patients treated with ICI-mono (P=0.009), but it was not associated with worse PFS in patients treated with ICI-chemo (P=0.132). The group treated with ICI-mono had worse PFS compared to the group treated with ICI-chemo in patients with max BTS ≥50 mm (P=0.004), and the group treated with ICI-mono was not associated with worse PFS compared to the group treated with ICI-chemo in patients with max BTS <50 mm (P=0.107).
While a large max BTS was identified as a prognostic factor for worse PFS in patients treated with ICI-mono, it was not identified as such in patients treated with ICI-chemo. The max BTS may have different predicting efficacy for patients with NSCLC treated with ICI-mono and ICI-chemo.
基线肿瘤大小(BTS)是接受免疫检查点抑制剂单药治疗(ICI-单药)的非小细胞肺癌(NSCLC)患者的一个预后因素。然而,在接受ICI联合化疗(ICI-化疗)治疗的患者中,这种关系尚不清楚。
这项单中心回顾性研究评估了2016年1月至2021年4月期间接受一线ICI-单药或ICI-化疗的159例晚期NSCLC患者。根据实体瘤疗效评价标准,通过放射学评估,使用最大BTS(max BTS)(最大靶病灶的最长直径)和总BTS(靶病灶最长直径之和)来估计他们的BTS值。
基于多变量分析,max BTS较大的组在接受ICI-单药治疗的患者中无进展生存期(PFS)较差(P=0.009),但在接受ICI-化疗的患者中与较差的PFS无关(P=0.132)。在max BTS≥50 mm的患者中,接受ICI-单药治疗的组比接受ICI-化疗的组PFS更差(P=0.004),而在max BTS<50 mm的患者中,接受ICI-单药治疗的组与接受ICI-化疗的组相比,PFS无明显差异(P=0.107)。
虽然较大的max BTS被确定为接受ICI-单药治疗患者PFS较差的一个预后因素,但在接受ICI-化疗的患者中并非如此。max BTS对接受ICI-单药和ICI-化疗治疗的NSCLC患者可能具有不同的预测效力。