Centre for Immunology of Infectious Diseases and Vaccines, National Institute for Public Health and the Environment (RIVM), Bilthoven, the Netherlands.
Centre for Immunology of Infectious Diseases and Vaccines, National Institute for Public Health and the Environment (RIVM), Bilthoven, the Netherlands.
Vaccine. 2022 Apr 1;40(15):2251-2257. doi: 10.1016/j.vaccine.2022.03.009. Epub 2022 Mar 9.
With COVID-19 vaccine roll-out ongoing in many countries globally, monitoring of breakthrough infections is of great importance. Antibodies persist in the blood after a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. Since COVID-19 vaccines induce immune response to the Spike protein of the virus, which is the main serosurveillance target to date, alternative targets should be explored to distinguish infection from vaccination.
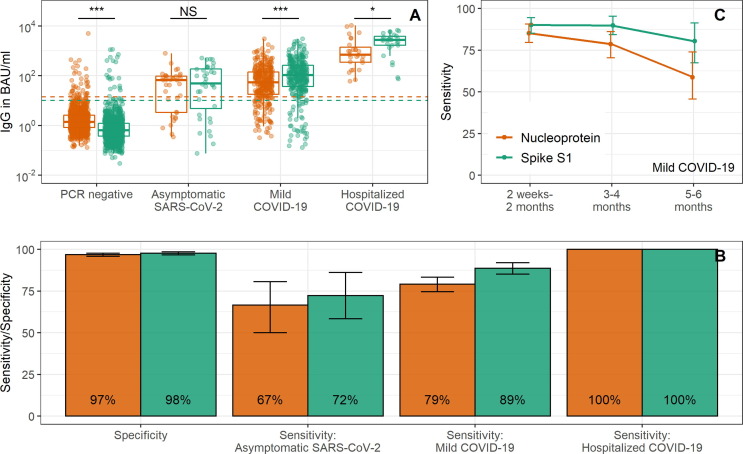
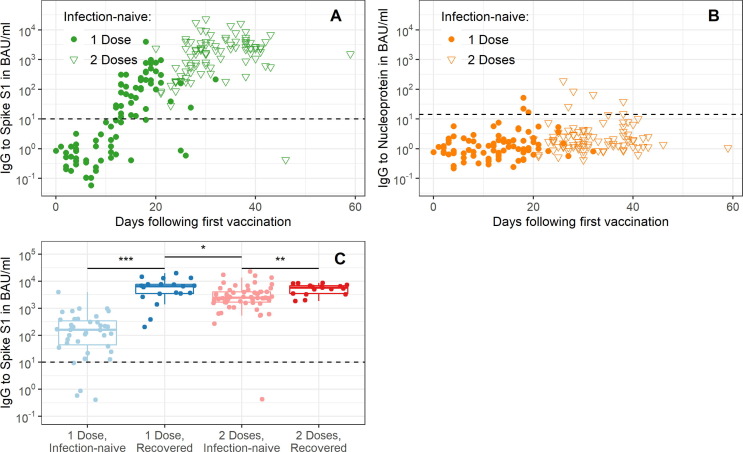
Multiplex immunoassay data from 1,513 SARS-CoV-2 RT-qPCR-tested individuals (352 positive and 1,161 negative) without COVID-19 vaccination history were used to determine the accuracy of Nucleoprotein-specific immunoglobulin G (IgG) in detecting past SARS-CoV-2 infection. We also described Spike S1 and Nucleoprotein-specific IgG responses in 230 COVID-19 vaccinated individuals (Pfizer/BioNTech).
The sensitivity of Nucleoprotein seropositivity was 85% (95% confidence interval: 80-90%) for mild COVID-19 in the first two months following symptom onset. Sensitivity was lower in asymptomatic individuals (67%, 50-81%). Participants who had experienced a SARS-CoV-2 infection up to 11 months preceding vaccination, as assessed by Spike S1 seropositivity or RT-qPCR, produced 2.7-fold higher median levels of IgG to Spike S1 ≥ 14 days after the first dose as compared to those unexposed to SARS-CoV-2 at ≥ 7 days after the second dose (p = 0.011). Nucleoprotein-specific IgG concentrations were not affected by vaccination in infection-naïve participants.
Serological responses to Nucleoprotein may prove helpful in identifying SARS-CoV-2 infections after vaccination. Furthermore, it can help interpret IgG to Spike S1 after COVID-19 vaccination as particularly high responses shortly after vaccination could be explained by prior exposure history.
随着 COVID-19 疫苗在全球许多国家的推出,对突破性感染的监测至关重要。严重急性呼吸系统综合症冠状病毒 2(SARS-CoV-2)感染后,抗体在血液中持续存在。由于 COVID-19 疫苗诱导针对病毒刺突蛋白的免疫反应,这是迄今为止主要的血清学监测目标,因此应探索替代靶标以区分感染和接种疫苗。
使用来自 1513 名未接种 COVID-19 疫苗且无 COVID-19 病史的 SARS-CoV-2 RT-qPCR 检测个体(352 例阳性和 1161 例阴性)的多重免疫分析数据,以确定核蛋白特异性免疫球蛋白 G(IgG)在检测过去 SARS-CoV-2 感染中的准确性。我们还描述了 230 名 COVID-19 接种者(辉瑞/生物技术)的刺突 S1 和核蛋白特异性 IgG 反应。
在症状出现后两个月内,核蛋白血清阳性的敏感性为轻度 COVID-19 的 85%(95%置信区间:80-90%)。无症状个体的敏感性较低(67%,50-81%)。通过 Spike S1 血清阳性或 RT-qPCR 评估,在接种疫苗前 11 个月内感染过 SARS-CoV-2 的参与者,与在接种疫苗前至少 7 天未接触 SARS-CoV-2 的参与者相比,在第一剂后至少 14 天,产生的 Spike S1 IgG 中位数水平高 2.7 倍(p=0.011)。在无感染史的参与者中,接种疫苗不会影响核蛋白特异性 IgG 浓度。
针对核蛋白的血清学反应可能有助于识别接种疫苗后的 SARS-CoV-2 感染。此外,它可以帮助解释 COVID-19 接种后 Spike S1 的 IgG,因为接种疫苗后不久出现的特别高的反应可以用先前的暴露史来解释。