Lancet. 2022 Apr 2;399(10332):1322-1335. doi: 10.1016/S0140-6736(21)02868-3. Epub 2022 Mar 13.
Previous Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) studies have reported national health estimates for Ethiopia. Substantial regional variations in socioeconomic status, population, demography, and access to health care within Ethiopia require comparable estimates at the subnational level. The GBD 2019 Ethiopia subnational analysis aimed to measure the progress and disparities in health across nine regions and two chartered cities.
We gathered 1057 distinct data sources for Ethiopia and all regions and cities that included census, demographic surveillance, household surveys, disease registry, health service use, disease notifications, and other data for this analysis. Using all available data sources, we estimated the Socio-demographic Index (SDI), total fertility rate (TFR), life expectancy, years of life lost, years lived with disability, disability-adjusted life-years, and risk-factor-attributable health loss with 95% uncertainty intervals (UIs) for Ethiopia's nine regions and two chartered cities from 1990 to 2019. Spatiotemporal Gaussian process regression, cause of death ensemble model, Bayesian meta-regression tool, DisMod-MR 2.1, and other models were used to generate fertility, mortality, cause of death, and disability rates. The risk factor attribution estimations followed the general framework established for comparative risk assessment.
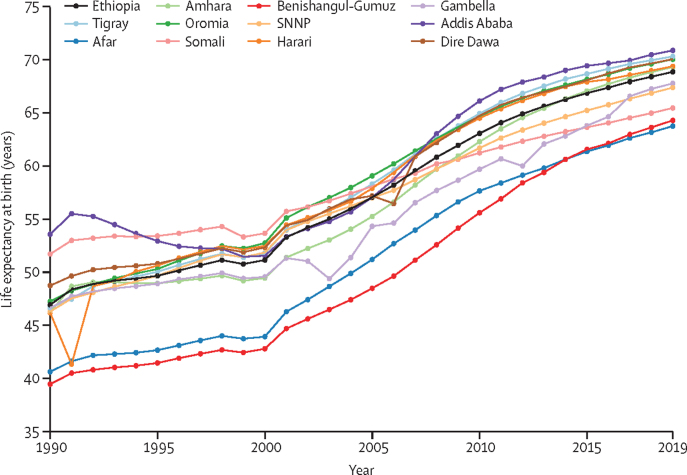
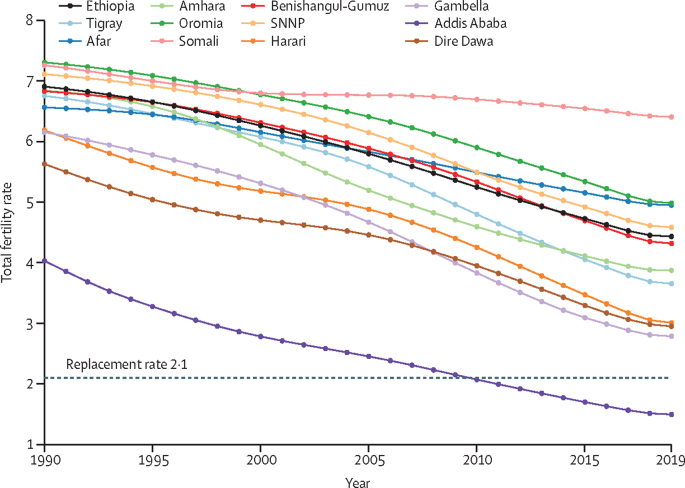
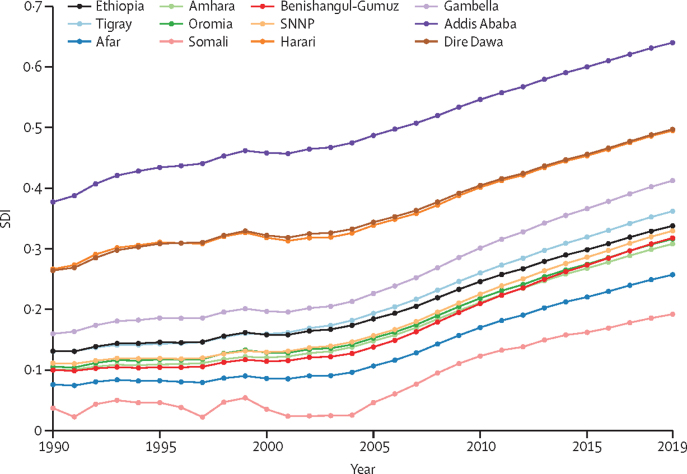
The SDI steadily improved in all regions and cities from 1990 to 2019, yet the disparity between the highest and lowest SDI increased by 54% during that period. The TFR declined from 6·91 (95% UI 6·59-7·20) in 1990 to 4·43 (4·01-4·92) in 2019, but the magnitude of decline also varied substantially among regions and cities. In 2019, TFR ranged from 6·41 (5·96-6·86) in Somali to 1·50 (1·26-1·80) in Addis Ababa. Life expectancy improved in Ethiopia by 21·93 years (21·79-22·07), from 46·91 years (45·71-48·11) in 1990 to 68·84 years (67·51-70·18) in 2019. Addis Ababa had the highest life expectancy at 70·86 years (68·91-72·65) in 2019; Afar and Benishangul-Gumuz had the lowest at 63·74 years (61·53-66·01) for Afar and 64.28 (61.99-66.63) for Benishangul-Gumuz. The overall increases in life expectancy were driven by declines in under-5 mortality and mortality from common infectious diseases, nutritional deficiency, and war and conflict. In 2019, the age-standardised all-cause death rate was the highest in Afar at 1353·38 per 100 000 population (1195·69-1526·19). The leading causes of premature mortality for all sexes in Ethiopia in 2019 were neonatal disorders, diarrhoeal diseases, lower respiratory infections, tuberculosis, stroke, HIV/AIDS, ischaemic heart disease, cirrhosis, congenital defects, and diabetes. With high SDIs and life expectancy for all sexes, Addis Ababa, Dire Dawa, and Harari had low rates of premature mortality from the five leading causes, whereas regions with low SDIs and life expectancy for all sexes (Afar and Somali) had high rates of premature mortality from the leading causes. In 2019, child and maternal malnutrition; unsafe water, sanitation, and handwashing; air pollution; high systolic blood pressure; alcohol use; and high fasting plasma glucose were the leading risk factors for health loss across regions and cities.
There were substantial improvements in health over the past three decades across regions and chartered cities in Ethiopia. However, the progress, measured in SDI, life expectancy, TFR, premature mortality, disability, and risk factors, was not uniform. Federal and regional health policy makers should match strategies, resources, and interventions to disease burden and risk factors across regions and cities to achieve national and regional plans, Sustainable Development Goals, and universal health coverage targets.
Bill & Melinda Gates Foundation.
之前的全球疾病、伤害和危险因素研究(GBD)报告了埃塞俄比亚的国家健康状况。埃塞俄比亚内部在社会经济地位、人口、人口统计和医疗保健获取方面存在显著的地区差异,因此需要在次国家级水平上进行可比的估计。GBD 2019 年埃塞俄比亚次国家级分析旨在衡量九个地区和两个特许城市的健康进展和差异。
我们收集了 1057 个埃塞俄比亚和所有地区和城市的独特数据源,包括人口普查、人口监测、家庭调查、疾病登记、医疗服务使用、疾病报告和其他数据,用于本次分析。我们使用所有可用的数据来源,估计了 1990 年至 2019 年埃塞俄比亚九个地区和两个特许城市的社会人口指数(SDI)、总生育率(TFR)、预期寿命、生命损失年数、残疾生存年数、残疾调整生命年数以及与风险因素相关的健康损失,置信区间(UI)为 95%。时空高斯过程回归、死因综合模型、贝叶斯荟萃回归工具、DisMod-MR 2.1 等模型用于生成生育率、死亡率、死因和残疾率。风险因素归因估计遵循比较风险评估的一般框架。
1990 年至 2019 年期间,所有地区和城市的 SDI 稳步提高,但期间最高和最低 SDI 之间的差距增加了 54%。TFR 从 1990 年的 6.91(95% UI 6.59-7.20)下降到 2019 年的 4.43(4.01-4.92),但各地区和城市的下降幅度也有很大差异。2019 年,TFR 范围从索马里的 6.41(5.96-6.86)到亚的斯亚贝巴的 1.50(1.26-1.80)。埃塞俄比亚的预期寿命提高了 21.93 年(21.79-22.07),从 1990 年的 46.91 岁(45.71-48.11)提高到 2019 年的 68.84 岁(67.51-70.18)。亚的斯亚贝巴的预期寿命最高,为 2019 年的 70.86 岁(68.91-72.65);阿法尔和本尚古勒-古马兹的预期寿命最低,阿法尔为 63.74 岁(61.53-66.01),本尚古勒-古马兹为 64.28 岁(61.99-66.63)。预期寿命的整体增长是由五岁以下死亡率和常见传染病、营养缺乏、战争和冲突导致的死亡率下降推动的。2019 年,阿法尔的全因死亡率最高,为 1353.38 人/100000 人(1195.69-1526.19)。埃塞俄比亚 2019 年所有性别的主要死亡原因是新生儿疾病、腹泻病、下呼吸道感染、结核病、中风、艾滋病毒/艾滋病、缺血性心脏病、肝硬化、先天性缺陷和糖尿病。由于阿法尔和索马里的社会人口指数和预期寿命都较低,所有性别的 5 大主要死亡原因导致的过早死亡率较高;而阿法尔和索马里的社会人口指数和预期寿命都较低,所有性别的 5 大主要死亡原因导致的过早死亡率较高。2019 年,儿童和孕产妇营养不良、不安全的水、环境卫生和手部卫生、空气污染、高血压、饮酒和高空腹血糖是各地区和城市健康损失的主要风险因素。
过去三十年,埃塞俄比亚各个地区和特许城市的健康状况都有了显著改善。然而,在 SDI、预期寿命、TFR、过早死亡率、残疾和风险因素方面的进展并不均衡。联邦和地区卫生政策制定者应根据疾病负担和风险因素在各地区和城市的情况,调整策略、资源和干预措施,以实现国家和地区计划、可持续发展目标和全民健康覆盖目标。
比尔及梅琳达·盖茨基金会。