Department of Cardiology, CARIM, Maastricht University Medical Centre, Maastricht, The Netherlands.
Netherlands Heart Institute (NLHI), Utrecht, The Netherlands.
ESC Heart Fail. 2022 Jun;9(3):2032-2036. doi: 10.1002/ehf2.13861. Epub 2022 Mar 17.
The HFA-PEFF score was developed to optimize diagnosis and to aid in early recognition of heart failure (HF) with preserved ejection fraction (HFpEF) in patients who present with HF-like symptoms. Recognizing early-HFpEF phenogroups is essential to better understand progression towards overt HFpEF and pave the way for early intervention and treatment. Whether the HFA-PEFF domain scores can identify 'early-HFpEF' phenogroups remains unknown. The aims of this pilot study are to (i) identify distinct phenogroups by cluster analysis of HFA-PEFF domain scores in subjects that present with HF-like symptoms and (ii) study whether these phenogroups may be associated with distinct blood proteome profiles.
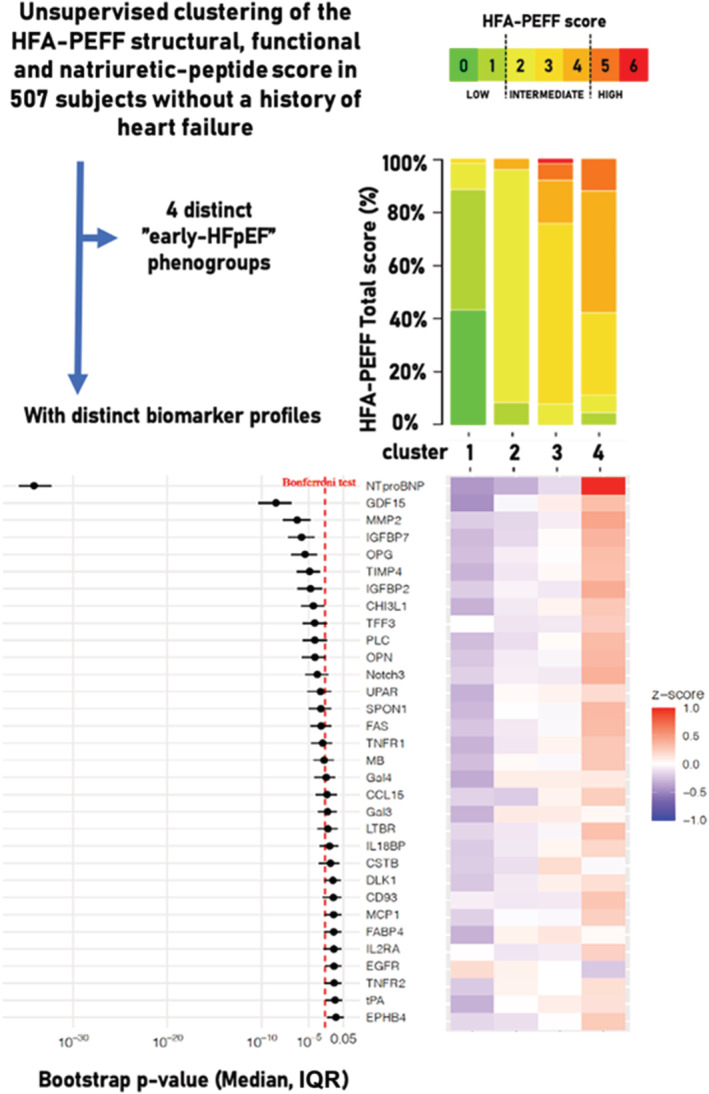
Subjects referred to the Cardiology Centers of the Netherlands, location Utrecht, with non-acute possibly cardiac-related symptoms (such as dyspnoea or fatigue) were prospectively enrolled in the HELPFul cohort (N = 507) and were included in the current analysis. Inclusion criteria for this study were (i) age ≥ 45 years and (ii) a left ventricular ejection fraction (LVEF) ≥ 50%, in the absence of a history of HF, coronary artery disease, congenital heart disease, or any previous cardiac interventions. Multinominal-based clustering with latent class model using the HFA-PEFF domain scores (functional, structural, and biomarker scores) as input was used to detect distinct phenotypic clusters. For each bootstrapping run, the 92 Olink proteins were analysed for their association with the identified phenogroups. Four distinct phenogroups were identified in the current analysis (validated by bootstrapping 1000×): (i) no left ventricular diastolic dysfunction (no LVDD, N = 102); (ii) LVDD with functional left ventricular (LV) abnormalities (N = 204); (iii) LVDD with functional and structural LV abnormalities (N = 204); and (iv) LVDD with functional and structural LV abnormalities and elevated BNP (N = 107). The HFA-PEFF total score risk categories significantly differed between the phenogroups (P < 0.001), with an increase of the HFA-PEFF score from Phenogroup 1 to 4 (low/intermediate/high HFA-PEFF risk score: Phenogroup 1: 88%/12%/0%; Phenogroup 2: 9%/91%/0%; Phenogroup 3: 0%/92%/8%; Phenogroup 4: 5%/83%/12%). Thirty-two out of the 92 Olink protein biomarkers significantly differed among the phenogroups. The top eight biomarkers-N-terminal prohormone brain natriuretic peptide, growth differentiation factor-15, matrix metalloproteinase-2, osteoprotegerin, tissue inhibitor of metalloproteinase-4, chitinase-3-like protein 1, insulin-like growth factor-binding protein 2, and insulin-like growth factor-binding protein 7-are mainly involved in inflammation and extracellular matrix remodelling, which are currently proposed key processes in HFpEF pathophysiology.
This study identified distinct phenogroups by using the HFA-PEFF domain scores in ambulant subjects referred for HF-like symptoms. The newly identified phenogroups accompanied by their circulating biomarkers profile might aid in a better understanding of the pathophysiological processes involved during the early stages of the HFpEF syndrome.
HFA-PEFF 评分旨在优化诊断并帮助早期识别射血分数保留的心力衰竭(HFpEF)患者的心力衰竭(HF),这些患者表现出类似 HF 的症状。识别早期 HFpEF 表型对于更好地了解向明显 HFpEF 的进展并为早期干预和治疗铺平道路至关重要。HFA-PEFF 域评分是否可以识别“早期 HFpEF”表型仍不清楚。本研究旨在(i)通过对出现类似 HF 症状的患者的 HFA-PEFF 域评分进行聚类分析来确定不同的表型组,以及(ii)研究这些表型组是否与不同的血液蛋白质组谱相关。
荷兰乌得勒支心脏病中心转诊的出现非急性可能与心脏相关症状(如呼吸困难或疲劳)的患者前瞻性纳入 HELPFul 队列(N=507),并纳入本分析。本研究的纳入标准为(i)年龄≥45 岁和(ii)左心室射血分数(LVEF)≥50%,无心力衰竭、冠状动脉疾病、先天性心脏病或任何先前的心脏干预史。使用基于多项的聚类分析和潜在类别模型,使用 HFA-PEFF 域评分(功能、结构和生物标志物评分)作为输入,以检测不同的表型聚类。对于每次引导运行,分析了 92 个 Olink 蛋白与鉴定的表型群之间的相关性。目前的分析确定了四个不同的表型群(通过引导 1000 次验证):(i)无左心室舒张功能障碍(无 LVDD,N=102);(ii)有 LVDD 和功能异常的左心室(LV)(N=204);(iii)有 LVDD 和功能和结构异常的 LV(N=204);和(iv)有 LVDD 和功能和结构异常以及升高的 BNP(N=107)。表型群之间 HFA-PEFF 总评分风险类别有显著差异(P<0.001),HFA-PEFF 评分从表型群 1 到 4 逐渐升高(低/中/高 HFA-PEFF 风险评分:表型群 1:88%/12%/0%;表型群 2:9%/91%/0%;表型群 3:0%/92%/8%;表型群 4:5%/83%/12%)。92 个 Olink 蛋白质生物标志物中有 32 个在表型群之间存在显著差异。前 8 个生物标志物-N 端脑利钠肽前体、生长分化因子 15、基质金属蛋白酶-2、骨保护素、基质金属蛋白酶抑制剂-4、几丁质酶-3 样蛋白 1、胰岛素样生长因子结合蛋白 2 和胰岛素样生长因子结合蛋白 7-主要参与炎症和细胞外基质重塑,这是目前提出的 HFpEF 病理生理学的关键过程。
本研究使用 HFA-PEFF 域评分在出现类似 HF 症状的门诊患者中确定了不同的表型群。新确定的表型群及其伴随的循环生物标志物谱可能有助于更好地了解 HFpEF 综合征早期阶段涉及的病理生理过程。