Sakuraya Masaaki, Douno Eri, Iwata Wakana, Takaba Akihiro, Hadama Kosuke, Kawamura Natsuki, Maezawa Toshinori, Iwamoto Kei, Yoshino Yuya, Yoshida Kenichi
Department of Emergency and Intensive Care Medicine, JA Hiroshima General Hospital, Jigozen 1-3-3, Hatsukaichi, Hiroshima, 738-8503, Japan.
Department of Emergency and Critical Care Medicine, Urasoe General Hospital, Okinawa, Japan.
J Intensive Care. 2022 Mar 18;10(1):17. doi: 10.1186/s40560-022-00603-w.
The end-tidal partial pressure of carbon dioxide (PCO) can be used to estimate the arterial partial pressure of carbon dioxide (PaCO) in patients who undergo mechanical ventilation via endotracheal intubation. However, no reliable method for measuring PCO during noninvasive ventilation (NIV) has been established. The purpose of this study was to evaluate the correlation and agreement between PaCO and PCO measured by these two methods and to compare them in patients who underwent NIV after extubation.
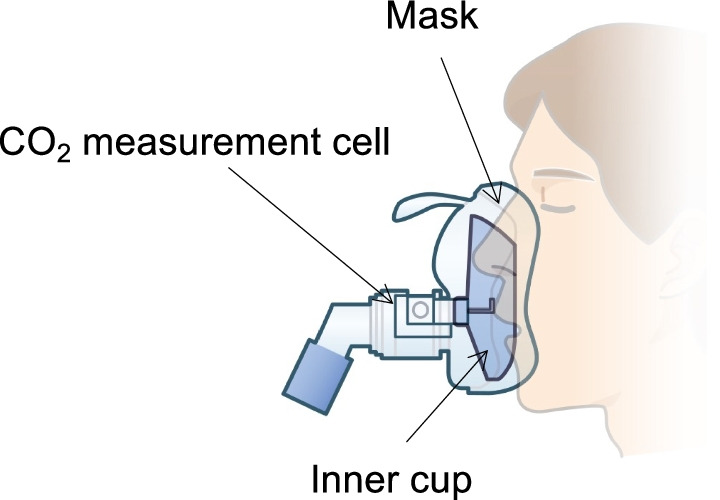
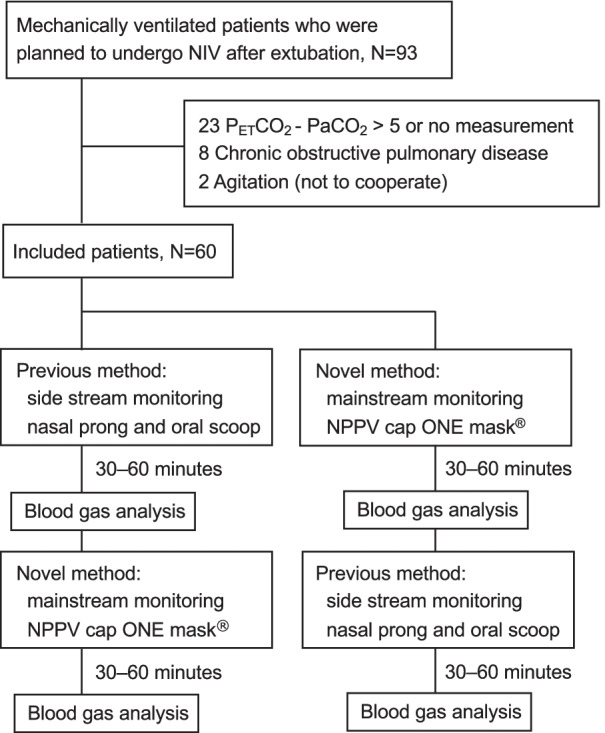
This study was a randomized, open-label, crossover trial in a mixed intensive care unit. We included patients who were planned for NIV after extubation and for whom the difference between PCO and PaCO was ≤ 5 mmHg. We compared mainstream capnography using an inner cup via face mask (the novel method) with sidestream capnography (the previous method) during NIV. The relationships between PaCO and PCO were evaluated by computing the Pearson correlation coefficient, and the agreement between PaCO and PCO was estimated using the Bland-Altman method.
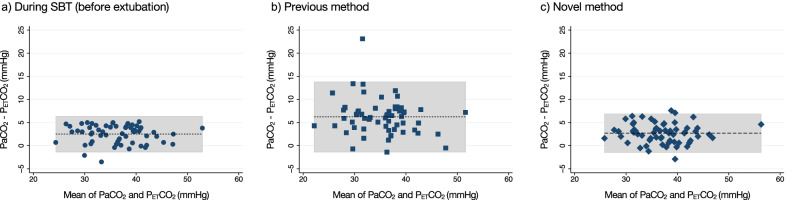
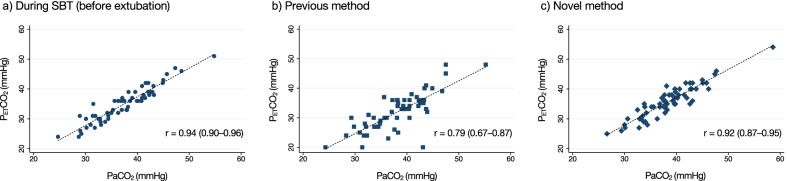
From April 2020 to October 2021, 60 patients were included to the study. PaCO and PCO were well correlated in both methods (the novel methods: r = 0.92, P < 0.001; the previous method: r = 0.79, P < 0.001). Mean bias between PaCO and PCO measured using the novel method was 2.70 (95% confidence interval [CI], 2.15-3.26) mmHg with 95% limits of agreement (LoA) ranging from - 1.61 to 7.02 mmHg, similar to the result of measurement during SBT (mean bias, 2.51; 95% CI, 2.00-3.02; 95% LoA, - 1.45 to 6.47 mmHg). In contrast, measurement using the previous method demonstrated a larger difference (mean bias, 6.22; 95% CI, 5.22-7.23; 95% LoA, - 1.54 to 13.99 mmHg).
The current study demonstrated that the novel PCO measurement was superior to the previous method for PaCO prediction. During NIV, the novel method may collect as sufficient exhalation sample as during intubation. Continuous PCO measurement combined with peripheral oxygen saturation monitoring is expected to be useful for early recognition of respiratory failure among high-risk patients after extubation. Trial registration UMIN-CTR UMIN000039459. Registered February 11, 2020.
对于经气管插管进行机械通气的患者,呼气末二氧化碳分压(PCO)可用于估计动脉血二氧化碳分压(PaCO)。然而,尚未建立在无创通气(NIV)期间测量PCO的可靠方法。本研究的目的是评估这两种方法测量的PaCO与PCO之间的相关性和一致性,并在拔管后接受NIV的患者中对它们进行比较。
本研究是在一个混合重症监护病房进行的随机、开放标签、交叉试验。我们纳入了计划在拔管后进行NIV且PCO与PaCO差值≤5 mmHg的患者。在NIV期间,我们将使用带内杯面罩的主流二氧化碳监测法(新方法)与旁流二氧化碳监测法(之前的方法)进行比较。通过计算Pearson相关系数评估PaCO与PCO之间的关系,并使用Bland-Altman方法估计PaCO与PCO之间的一致性。
从2020年4月至2021年10月,60例患者纳入本研究。两种方法中PaCO与PCO均具有良好的相关性(新方法:r = 0.92,P < 0.001;之前的方法:r = 0.79,P < 0.001)。使用新方法测量的PaCO与PCO之间的平均偏差为2.70(95%置信区间[CI],2.15 - 3.26)mmHg,95%一致性界限(LoA)范围为 - 1.61至7.02 mmHg,与自主呼吸试验期间的测量结果相似(平均偏差,2.51;95% CI,2.00 - 3.02;95% LoA, - 1.45至6.47 mmHg)。相比之下,使用之前的方法测量显示出更大的差异(平均偏差,6.22;95% CI,5.22 - 7.23;95% LoA, - 1.54至13.99 mmHg)。
本研究表明,新的PCO测量方法在预测PaCO方面优于之前的方法。在NIV期间,新方法可能收集到与插管期间一样充足的呼气样本。持续的PCO测量结合外周血氧饱和度监测有望有助于早期识别拔管后高危患者的呼吸衰竭。试验注册UMIN-CTR UMIN000039459。于2020年2月11日注册。