Pulmonary and Critical Care, Walter Reed National Military Medical Center, Bethesda, Maryland, USA.
Service de Pneumologie et Soins Intensifs, Hopital Europeen Georges Pompidou, Paris, France.
Thorax. 2023 Apr;78(4):368-375. doi: 10.1136/thoraxjnl-2021-218440. Epub 2022 Mar 24.
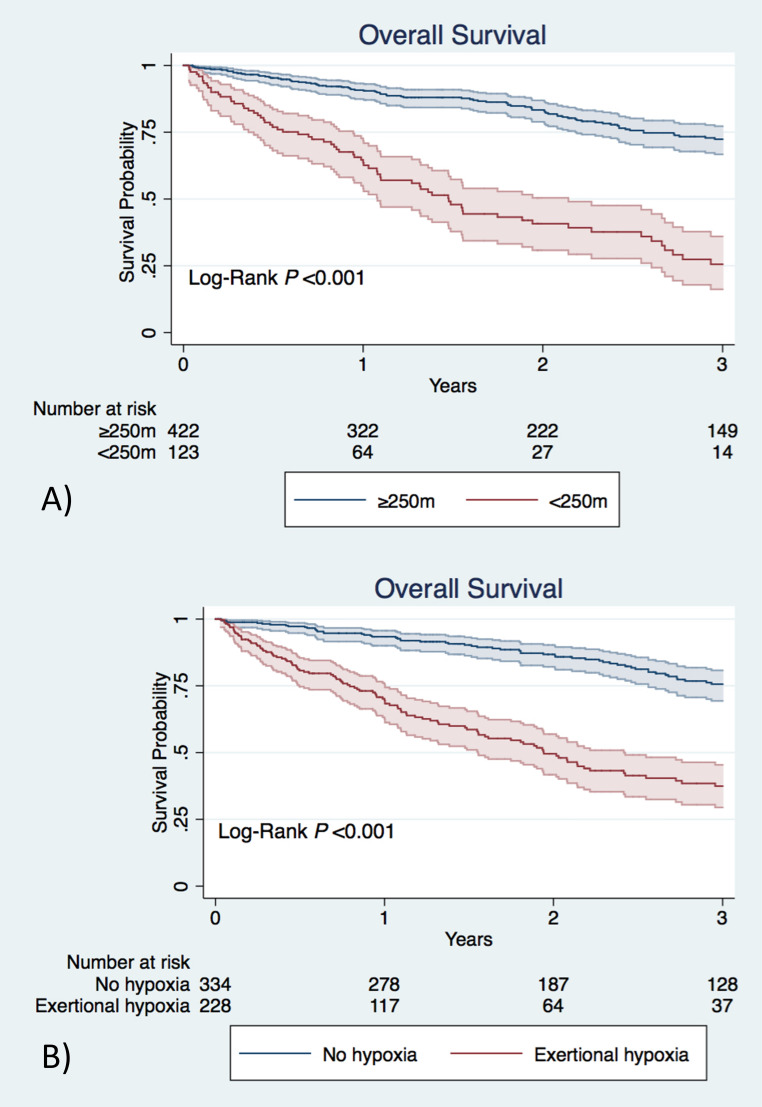
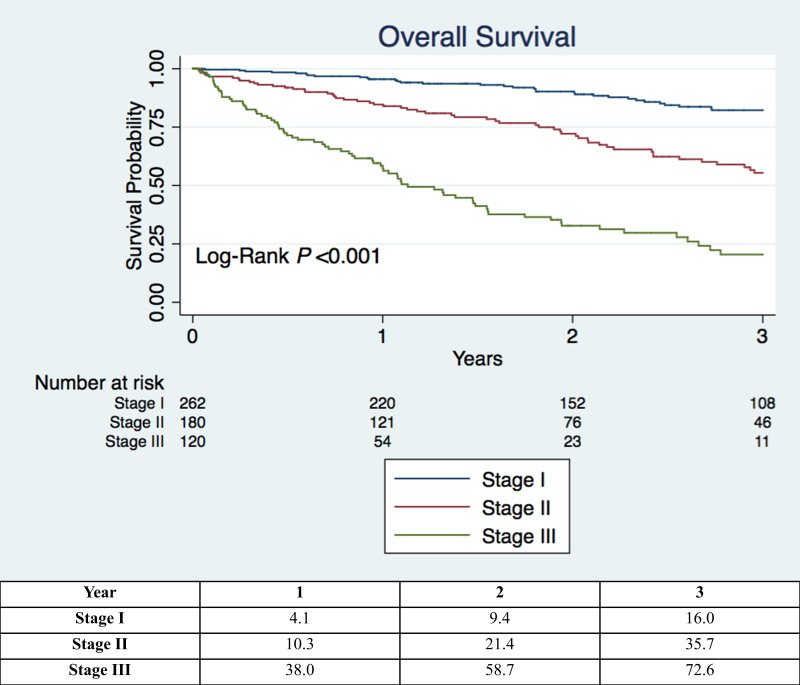
The gender-age-physiology (GAP) index is an easy-to-use baseline mortality prediction model in idiopathic pulmonary fibrosis (IPF). The GAP index does not incorporate exercise capacity parameters such as 6 min walk distance (6MWD) or exertional hypoxia. We evaluated if the addition of 6MWD and exertional hypoxia to the GAP index improves survival prediction in IPF.
Patients with IPF were identified at a tertiary care referral centre. Discrimination and calibration of the original GAP index were assessed. The cohort was then randomly divided into a derivation and validation set and performance of the GAP index with the addition of 6MWD and exertional hypoxia was evaluated. A final model was selected based on improvement in discrimination. Application of this model was then evaluated in a geographically distinct external cohort.
There were 562 patients with IPF identified in the internal cohort. Discrimination of the original GAP index was measured by a C-statistic of 0.676 (95% CI 0.635 to 0.717) and overestimated observed risk. 6MWD and exertional hypoxia were strongly predictive of mortality. The addition of these variables to the GAP index significantly improved model discrimination. A revised index incorporating exercise capacity parameters was constructed and performed well in the internal validation set (C-statistic: 0.752; 95% CI 0.701 to 0.802, difference in C-statistic compared with the refit GAP index: 0.050; 95% CI 0.004 to 0.097) and external validation set (N=108 (C-statistic: 0.780; 95% CI 0.682 to 0.877)).
A simple point-based baseline-risk prediction model incorporating exercise capacity predictors into the original GAP index may improve prognostication in patients with IPF.
性别-年龄-生理指数(GAP)是一种易于使用的特发性肺纤维化(IPF)基线死亡率预测模型。GAP 指数不包含运动能力参数,如 6 分钟步行距离(6MWD)或运动性低氧血症。我们评估了在 GAP 指数中加入 6MWD 和运动性低氧血症是否能改善 IPF 患者的生存预测。
在三级转诊中心确定 IPF 患者。评估原始 GAP 指数的区分度和校准度。然后,将队列随机分为推导和验证集,并评估加入 6MWD 和运动性低氧血症后 GAP 指数的性能。根据区分度的提高选择最终模型。然后在地理位置不同的外部队列中评估该模型的应用。
内部队列中确定了 562 名 IPF 患者。原始 GAP 指数的区分度通过 C 统计量 0.676(95%CI 0.635 至 0.717)进行测量,且高估了观察到的风险。6MWD 和运动性低氧血症对死亡率有很强的预测性。将这些变量加入 GAP 指数显著提高了模型的区分度。构建了一个包含运动能力参数的修订指数,在内部验证集(C 统计量:0.752;95%CI 0.701 至 0.802,与重新拟合 GAP 指数相比的 C 统计量差异:0.050;95%CI 0.004 至 0.097)和外部验证集(N=108(C 统计量:0.780;95%CI 0.682 至 0.877))中表现良好。
一种简单的基于点的基线风险预测模型,将运动能力预测因子纳入原始 GAP 指数,可能会改善 IPF 患者的预后。