Biochemistry Service, Vall d'Hebron Hospital, Autonomous University of Barcelona (UAB), Barcelona, Spain.
Cell Signaling and Cancer Progression Laboratory, Vall d'Hebron Institute of Research (VHIR), Barcelona, Spain.
BMC Med. 2022 Mar 29;20(1):129. doi: 10.1186/s12916-022-02345-w.
SARS-CoV-2 infection portends a broad range of outcomes, from a majority of asymptomatic cases to a lethal disease. Robust correlates of severe COVID-19 include old age, male sex, poverty, and co-morbidities such as obesity, diabetes, and cardiovascular disease. A precise knowledge of the molecular and biological mechanisms that may explain the association of severe disease with male sex is still lacking. Here, we analyzed the relationship of serum testosterone levels and the immune cell skewing with disease severity in male COVID-19 patients.
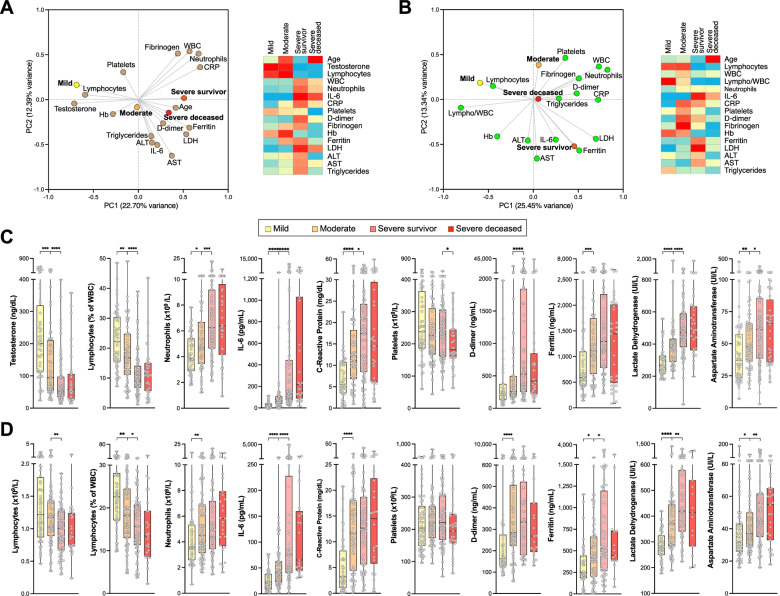
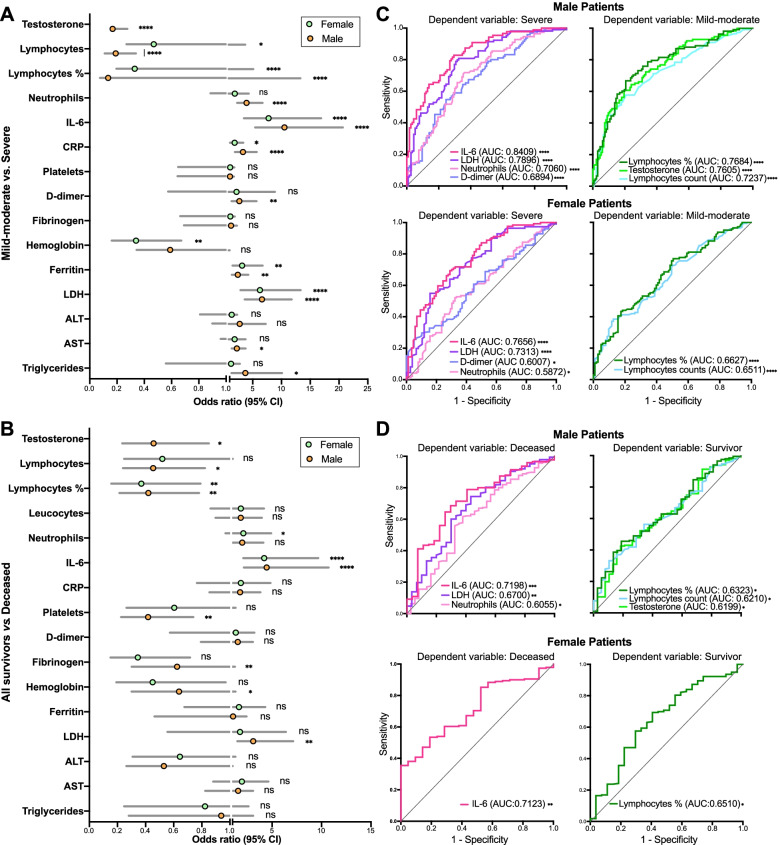
Biochemical and hematological parameters of admission samples in 497 hospitalized male and female COVID-19 patients, analyzed for associations with outcome and sex. Longitudinal (in-hospital course) analyses of a subcohort of 114 male patients were analyzed for associations with outcome. Longitudinal analyses of immune populations by flow cytometry in 24 male patients were studied for associations with outcome.
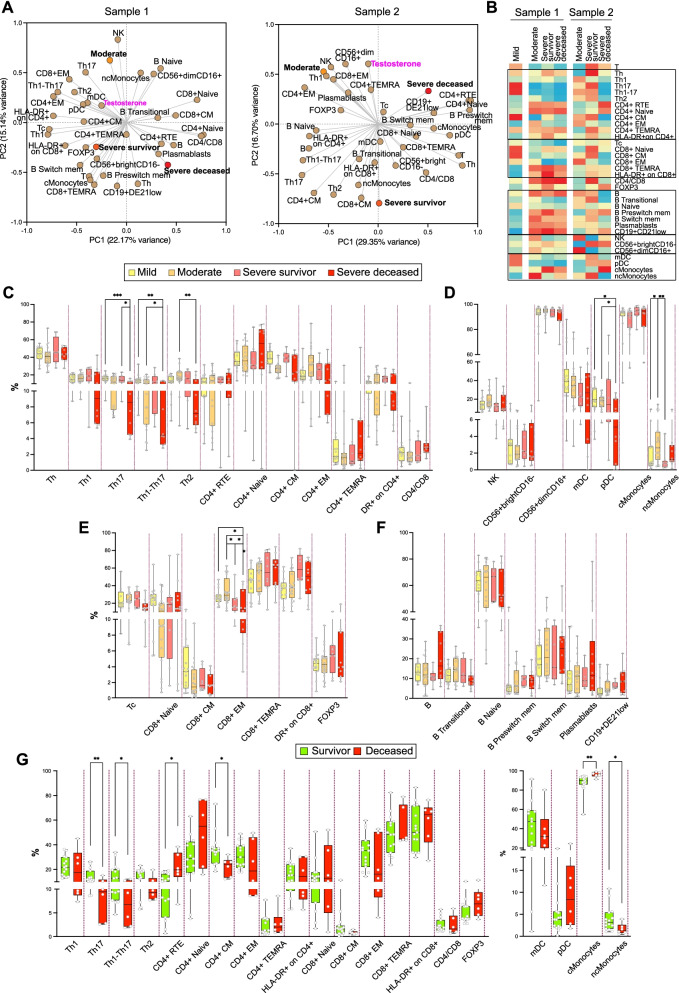
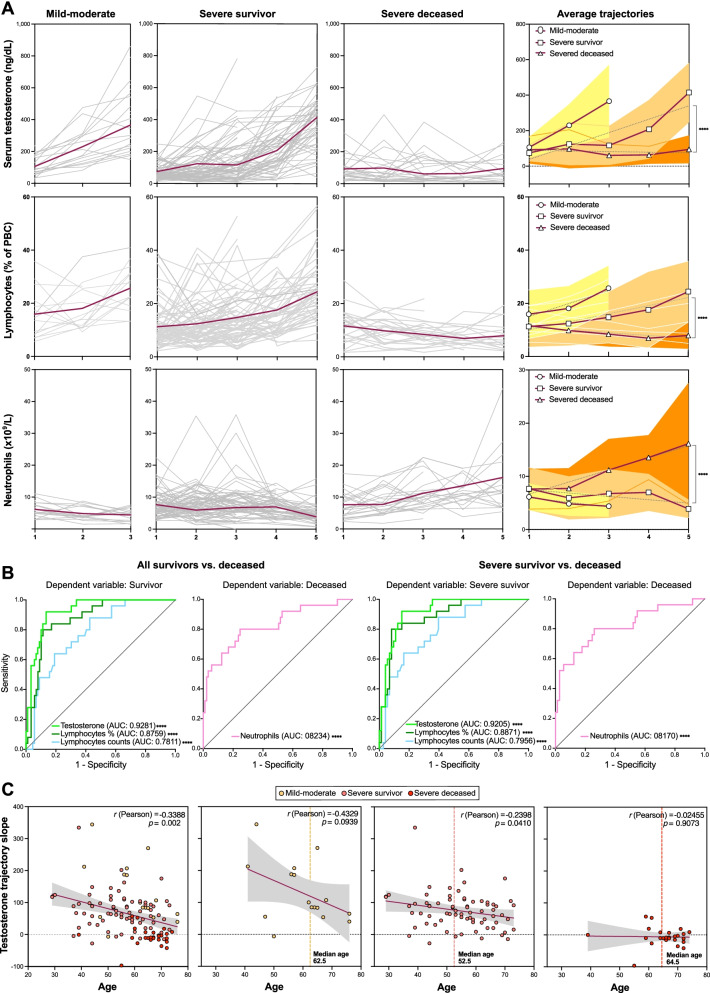
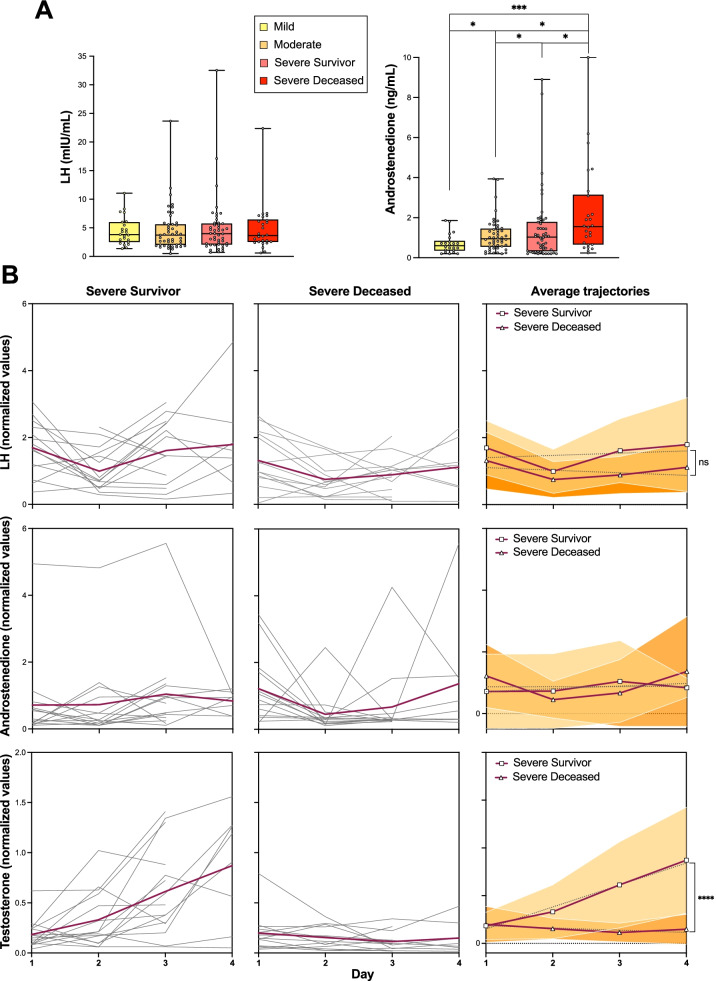
We have found quantitative differences in biochemical predictors of disease outcome in male vs. female patients. Longitudinal analyses in a subcohort of male COVID-19 patients identified serum testosterone trajectories as the strongest predictor of survival (AUC of ROC = 92.8%, p < 0.0001) in these patients among all biochemical parameters studied, including single-point admission serum testosterone values. In lethal cases, longitudinal determinations of serum luteinizing hormone (LH) and androstenedione levels did not follow physiological feedback patterns. Failure to reinstate physiological testosterone levels was associated with evidence of impaired T helper differentiation and augmented circulating classical monocytes.
Recovery or failure to reinstate testosterone levels is strongly associated with survival or death, respectively, from COVID-19 in male patients. Our data suggest an early inhibition of the central LH-androgen biosynthesis axis in a majority of patients, followed by full recovery in survivors or a peripheral failure in lethal cases. These observations are suggestive of a significant role of testosterone status in the immune responses to COVID-19 and warrant future experimental explorations of mechanistic relationships between testosterone status and SARS-CoV-2 infection outcomes, with potential prophylactic or therapeutic implications.
SARS-CoV-2 感染预示着广泛的结局,从大多数无症状病例到致命疾病。COVID-19 严重程度的可靠相关因素包括年龄较大、男性、贫困以及肥胖、糖尿病和心血管疾病等合并症。对于可能解释严重疾病与男性之间关联的分子和生物学机制,我们仍然知之甚少。在这里,我们分析了血清睾丸酮水平和免疫细胞倾斜与男性 COVID-19 患者疾病严重程度的关系。
分析了 497 名住院的男性和女性 COVID-19 患者入院样本的生化和血液学参数,以分析与结局和性别的关联。对 114 名男性患者的亚组进行了纵向(住院过程)分析,以分析与结局的关联。对 24 名男性患者的免疫群体进行了流式细胞术的纵向分析,以研究与结局的关联。
我们发现了男性与女性患者疾病结局的生化预测因素存在定量差异。在 COVID-19 男性患者的亚组中进行的纵向分析确定了血清睾丸酮轨迹是所有研究的生化参数中最强的生存预测因素(ROC 的 AUC = 92.8%,p < 0.0001),包括单点入院时的血清睾丸酮值。在致死病例中,血清黄体生成素(LH)和雄烯二酮水平的纵向测定没有遵循生理反馈模式。未能恢复生理睾丸酮水平与 T 辅助分化受损和循环经典单核细胞增加有关。
在男性患者中,睾丸酮水平的恢复或未能恢复与 COVID-19 的生存或死亡分别密切相关。我们的数据表明,大多数患者的中央 LH-雄激素生物合成轴早期受到抑制,随后幸存者恢复,而致死病例则外周衰竭。这些观察结果提示睾丸酮状态在 COVID-19 的免疫反应中具有重要作用,需要进一步探索睾丸酮状态与 SARS-CoV-2 感染结局之间的机制关系,这可能具有预防或治疗意义。