Michaelsen Maren M, Esch Tobias
Institute for Integrative Health Care and Health Promotion, Faculty of Health, Witten/Herdecke University, Witten, Germany.
Front Psychol. 2022 Mar 18;13:725644. doi: 10.3389/fpsyg.2022.725644. eCollection 2022.
Health behavior change is among the top recommendations for improving health of patients with lifestyle-related chronic diseases. An array of behavior change techniques (BCTs) have been developed to support behavior change initiation and maintenance. These BCTs often show limited success when they are not informed by theory, leading to a mismatch between the intention of the BCT and patients' needs or expectations. Previous studies have identified a number of resources (domains) which patients may require to initiate and maintain health behavior change. Indeed, not yet well established is how BCTs address these resources, i.e., the functional mechanisms of BCTs.
Provide a theoretical framework of the functional mechanisms of BCTs for developing and implementing successful interventions for health behavior change.
Conceptual review, including literature analysis and synthesis as well as conceptualization of a new model based on the synthesis.
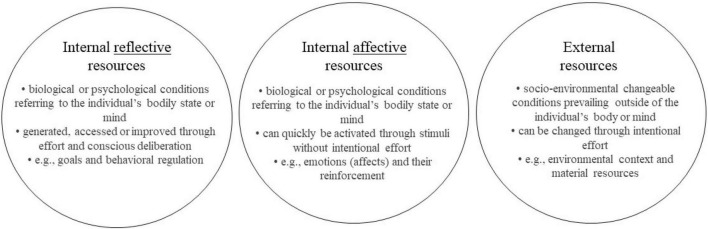
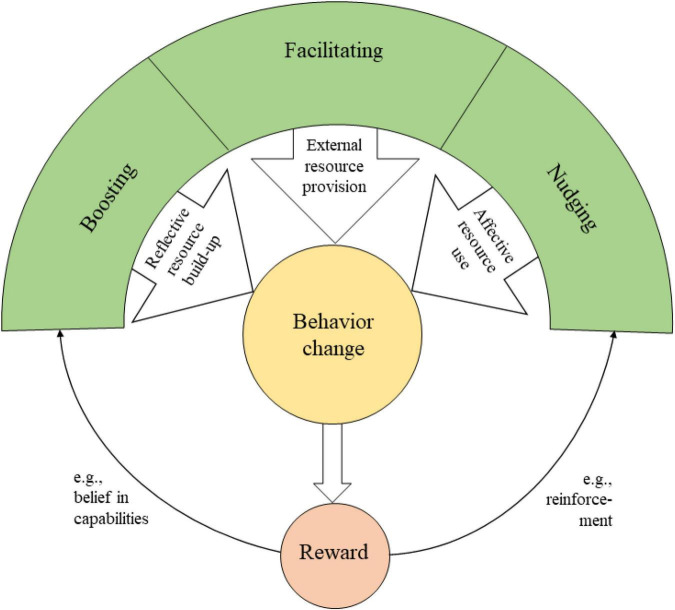
Through the integration of dual-process models as well as reward and motivation proceeding, i.e., affective, emotional, or intuitive neurobiological cues, into the rational framework of rather linear cognitive or task-related decision progress, we categorize previously identified resources into three distinct sets: external, internal reflective, and internal affective resources. Based on this triad, we classify BCTs according to their functional mechanisms into facilitating (=providing external resources), boosting (=strengthening internal reflective resources), and nudging (=activating internal affective resources). Consequently, we present a simplified Behavior Change Resource Model (BCRM) that is centered on patients' resources.
The model can be applied to develop health behavior change interventions, which promote engagement and empowerment. Future studies should aim at testing the applicability and practicality of the BCRM.
健康行为改变是改善与生活方式相关的慢性病患者健康状况的首要建议之一。为支持行为改变的启动和维持,已开发出一系列行为改变技术(BCTs)。当这些BCTs缺乏理论依据时,往往成效有限,导致BCTs的意图与患者的需求或期望不匹配。先前的研究已经确定了患者在启动和维持健康行为改变时可能需要的一些资源(领域)。事实上,BCTs如何利用这些资源,即BCTs的功能机制,尚未得到充分确立。
提供一个BCTs功能机制的理论框架,用于开发和实施成功的健康行为改变干预措施。
概念性综述,包括文献分析与综合,以及基于综合结果构建新模型的概念化过程。
通过将双过程模型以及奖励和动机过程,即情感、情绪或直觉神经生物学线索,整合到相对线性的认知或任务相关决策过程的理性框架中,我们将先前确定的资源分为三个不同的类别:外部资源、内部反思资源和内部情感资源。基于这一三元组,我们根据其功能机制将BCTs分为促进型(=提供外部资源)、增强型(=强化内部反思资源)和推动型(=激活内部情感资源)。因此,我们提出了一个以患者资源为核心的简化行为改变资源模型(BCRM)。
该模型可用于开发促进参与和赋权的健康行为改变干预措施。未来的研究应致力于测试BCRM的适用性和实用性。