Clinical Physiology, Department of Clinical Sciences Lund, Lund University, Skåne University Hospital, Lund, Sweden.
Wallenberg Centre for Molecular Medicine, Lund University, Lund, Sweden.
Pediatr Cardiol. 2022 Oct;43(7):1631-1644. doi: 10.1007/s00246-022-02894-0. Epub 2022 Apr 9.
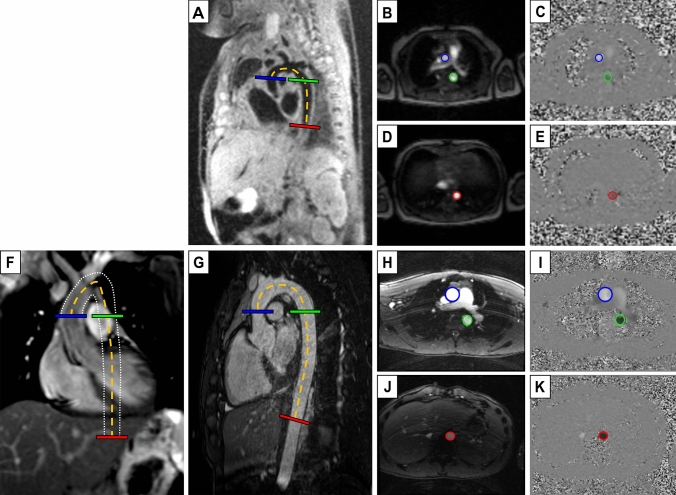
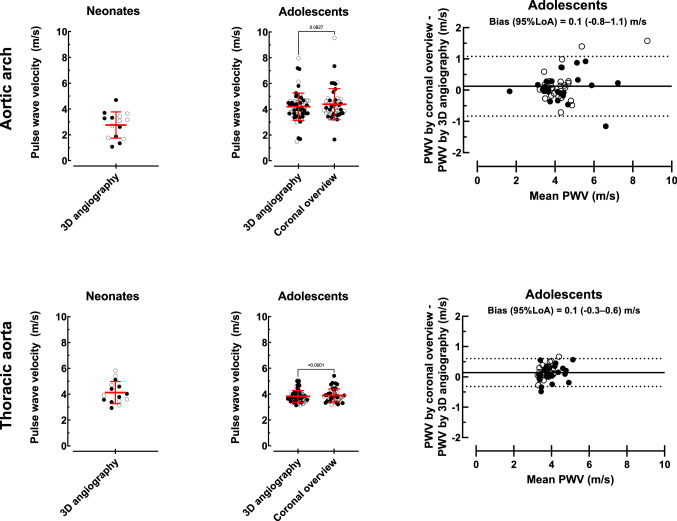
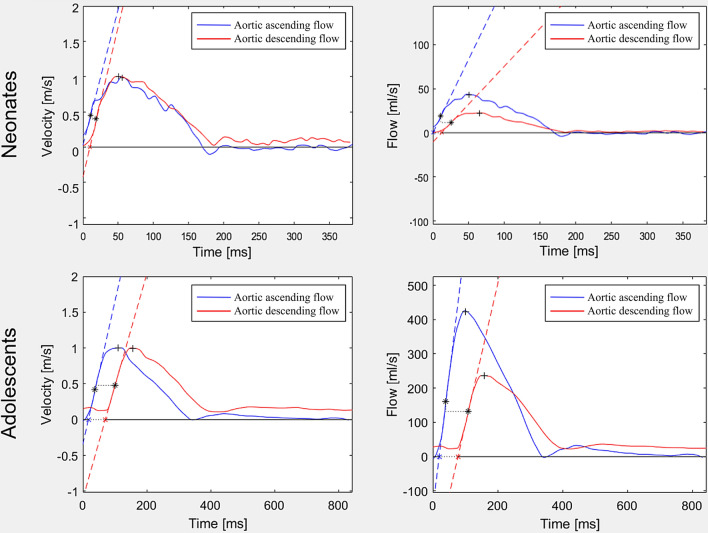
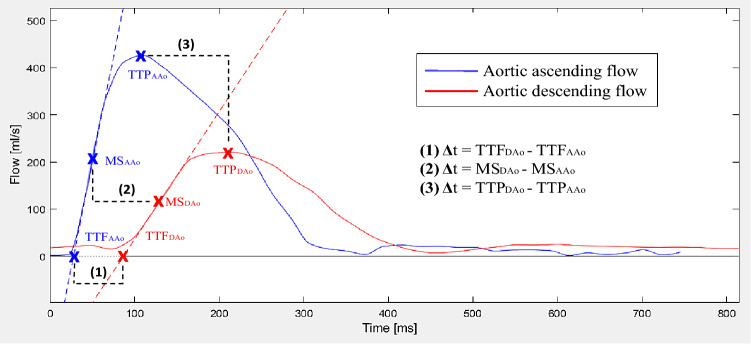
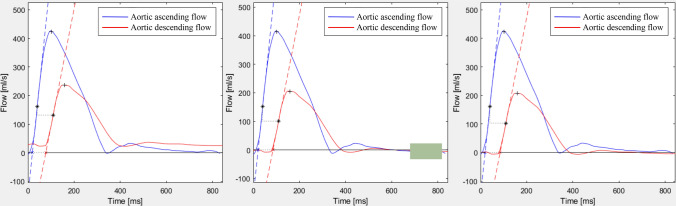
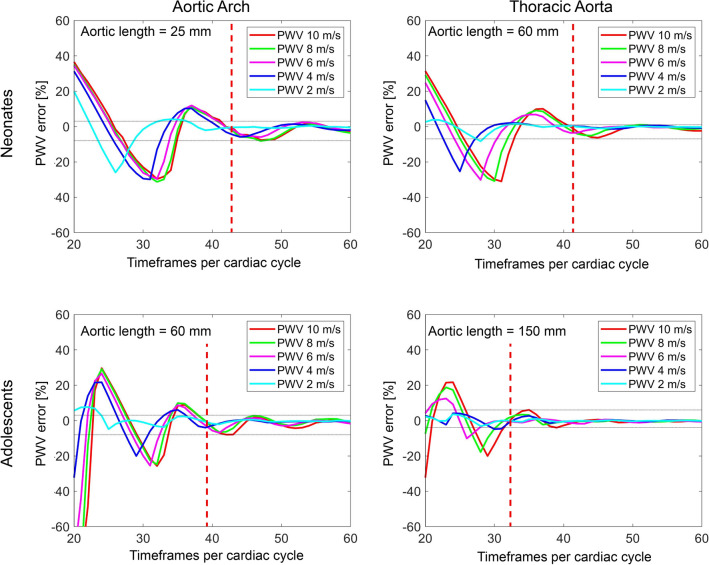
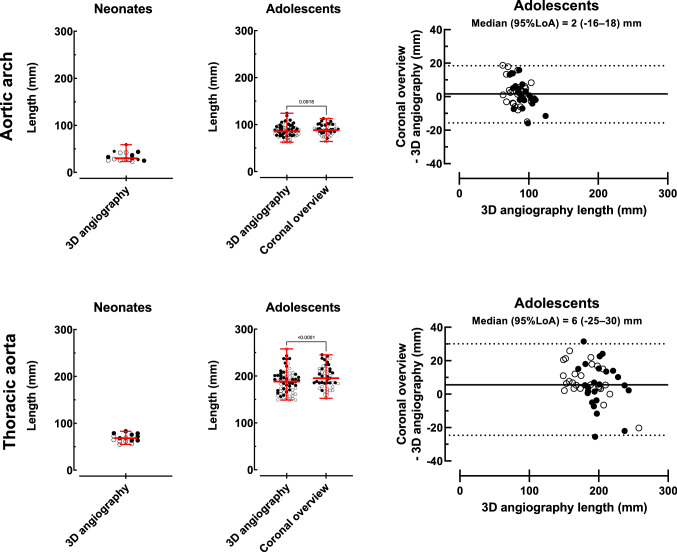
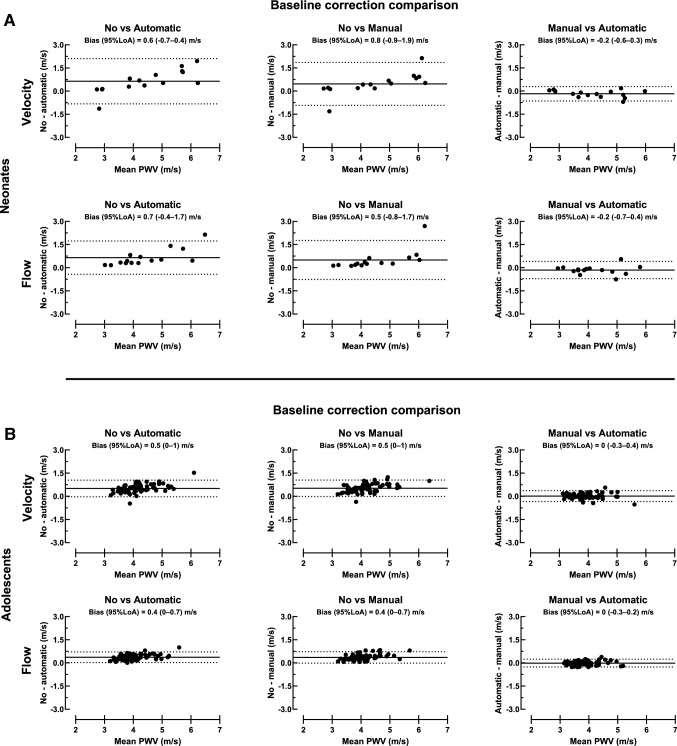
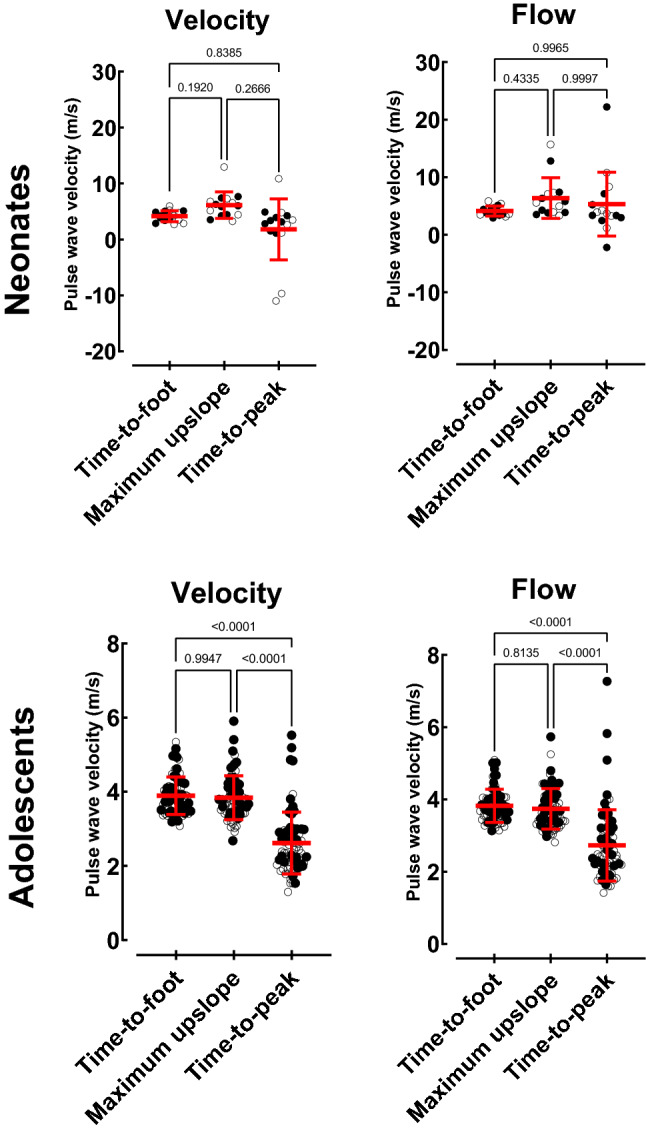
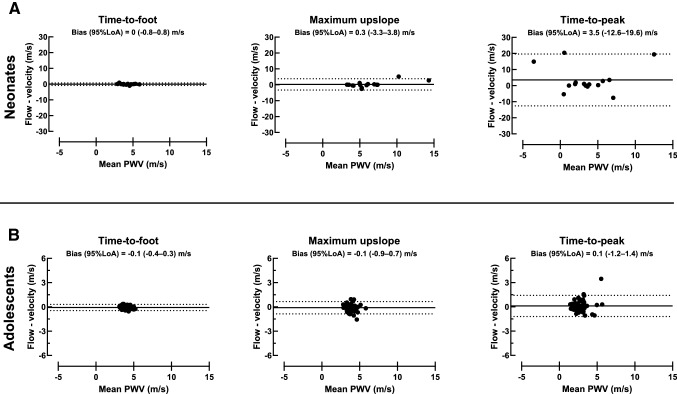
Pulse wave velocity (PWV) by cardiovascular magnetic resonance (CMR) lacks standardization. The aim of this study was to investigate methodological aspects of PWV measurements by CMR in neonates and adolescents. A computer phantom was created to validate the temporal resolution required for accurate PWV. Fifteen neonates and 71 adolescents underwent CMR with reference standard 3D angiography and phase-contrast flow acquisitions, and in a subset coronal overview images. Velocity and flow curves, transit time methods (time-to-foot (TTF), maximum upslope, and time-to-peak (TTP)), and baseline correction methods (no correction, automatic and manual) were investigated. In neonates, required timeframes per cardiac cycle for accurate PWV was 42 for the aortic arch and 41 for the thoracic aorta. In adolescents, corresponding values were 39 and 32. Aortic length differences by overview images and 3D angiography in adolescents were - 16-18 mm (aortic arch) and - 25-30 mm (thoracic aorta). Agreement in PWV between automatic and manual baseline correction was - 0.2 ± 0.3 m/s in neonates and 0.0 ± 0.1 m/s in adolescents. Velocity and flow-derived PWV measurements did not differ in either group (all p > 0.08). In neonates, transit time methods did not differ (all p > 0.19) but in adolescents PWV was higher for TTF (3.8 ± 0.5 m/s) and maximum upslope (3.7 ± 0.6 m/s) compared to TTP (2.7 ± 1.0 m/s; p < 0.0001). This study is a step toward standardization of PWV in neonates and adolescents using CMR. It provides required temporal resolution for phase-contrast flow acquisitions for typical heartrates in neonates and adolescents, and supports 3D angiography and time-to-foot with automatic baseline correction for accurate PWV measurements.
脉搏波速度(PWV)通过心血管磁共振(CMR)缺乏标准化。本研究旨在探讨新生儿和青少年 CMR 测量 PWV 的方法学方面。创建了一个计算机模型来验证准确测量 PWV 所需的时间分辨率。15 名新生儿和 71 名青少年接受 CMR 检查,同时进行参考标准 3D 血管造影和相位对比流量采集,并在亚组中进行冠状概述图像。测量了速度和流量曲线、渡越时间法(时间到脚(TTF)、最大上升斜率和到达峰值时间(TTP))以及基线校正方法(无校正、自动和手动)。在新生儿中,准确测量 PWV 所需的每个心动周期的时间框架为主动脉弓 42 个和胸主动脉 41 个。在青少年中,相应的值分别为 39 和 32。青少年通过概述图像和 3D 血管造影的主动脉长度差异为-16-18mm(主动脉弓)和-25-30mm(胸主动脉)。在新生儿中,自动和手动基线校正的 PWV 之间的一致性为-0.2±0.3m/s,在青少年中为 0.0±0.1m/s。在两组中,速度和流量衍生的 PWV 测量值均无差异(均 p>0.08)。在新生儿中,渡越时间法没有差异(均 p>0.19),但在青少年中,TTF(3.8±0.5m/s)和最大上升斜率(3.7±0.6m/s)的 PWV 高于 TTP(2.7±1.0m/s;p<0.0001)。本研究是朝着使用 CMR 对新生儿和青少年 PWV 标准化迈出的一步。它为新生儿和青少年典型心率的相位对比流量采集提供了所需的时间分辨率,并支持 3D 血管造影和时间到脚,自动基线校正可实现准确的 PWV 测量。