Dinoto Alessandro, Sechi Elia, Flanagan Eoin P, Ferrari Sergio, Solla Paolo, Mariotto Sara, Chen John J
Neurology Unit, Department of Neuroscience, Biomedicine and Movement Sciences, University of Verona, Verona, Italy.
Department of Medical, Surgical and Experimental Sciences, University of Sassari, Sassari, Italy.
Front Neurol. 2022 Mar 23;13:866824. doi: 10.3389/fneur.2022.866824. eCollection 2022.
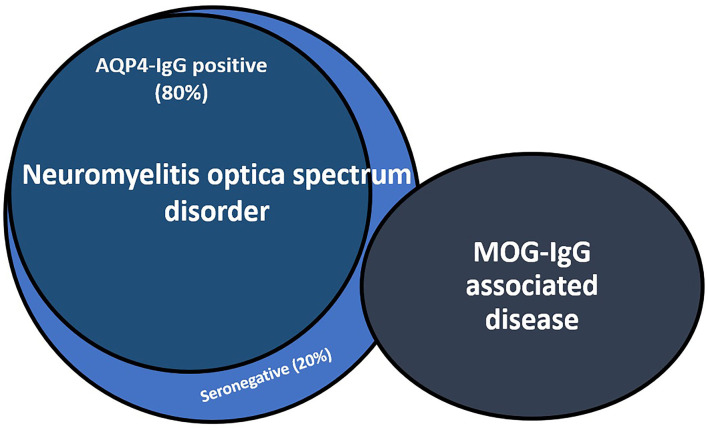
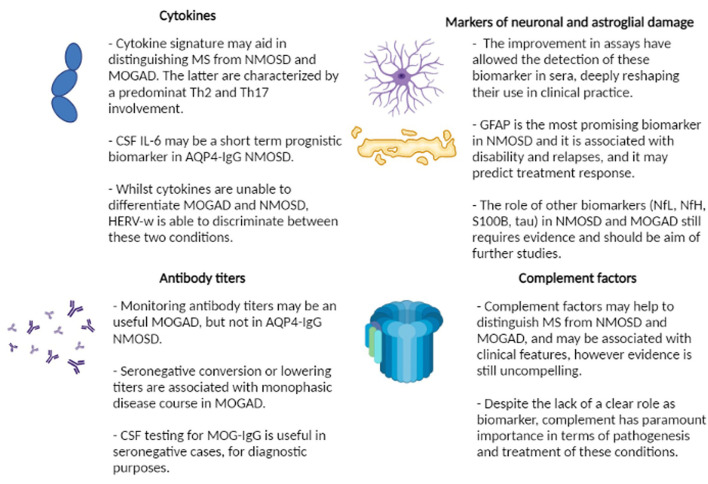
The term neuromyelitis optica spectrum disorder (NMOSD) describes a group of clinical-MRI syndromes characterized by longitudinally extensive transverse myelitis, optic neuritis, brainstem dysfunction and/or, less commonly, encephalopathy. About 80% of patients harbor antibodies directed against the water channel aquaporin-4 (AQP4-IgG), expressed on astrocytes, which was found to be both a biomarker and a pathogenic cause of NMOSD. More recently, antibodies against myelin oligodendrocyte glycoprotein (MOG-IgG), have been found to be a biomarker of a different entity, termed MOG antibody-associated disease (MOGAD), which has overlapping, but different pathogenesis, clinical features, treatment response, and prognosis when compared to AQP4-IgG-positive NMOSD. Despite important refinements in the accuracy of AQP4-IgG and MOG-IgG testing assays, a small proportion of patients with NMOSD still remain negative for both antibodies and are called "seronegative" NMOSD. Whilst major advances have been made in the diagnosis and treatment of these conditions, biomarkers that could help predict the risk of relapses, disease activity, and prognosis are still lacking. In this context, a number of serum and/or cerebrospinal fluid biomarkers are emerging as potentially useful in clinical practice for diagnostic and treatment purposes. These include antibody titers, cytokine profiles, complement factors, and markers of neuronal (e.g., neurofilament light chain) or astroglial (e.g., glial fibrillary acidic protein) damage. The aim of this review is to summarize current evidence regarding the role of emerging diagnostic and prognostic biomarkers in patients with NMOSD and MOGAD.
视神经脊髓炎谱系障碍(NMOSD)这一术语描述了一组临床-磁共振成像综合征,其特征为纵向广泛横贯性脊髓炎、视神经炎、脑干功能障碍和/或较少见的脑病。约80%的患者体内存在针对水通道蛋白4(AQP4-IgG)的抗体,该蛋白在星形胶质细胞上表达,被发现既是NMOSD的生物标志物,也是其致病原因。最近,针对髓鞘少突胶质细胞糖蛋白(MOG-IgG)的抗体被发现是一种不同疾病实体的生物标志物,称为MOG抗体相关疾病(MOGAD),与AQP4-IgG阳性的NMOSD相比,它具有重叠但不同的发病机制、临床特征、治疗反应和预后。尽管AQP4-IgG和MOG-IgG检测方法的准确性有了重要改进,但仍有一小部分NMOSD患者这两种抗体检测均为阴性,被称为“血清阴性”NMOSD。虽然在这些疾病的诊断和治疗方面取得了重大进展,但仍缺乏有助于预测复发风险、疾病活动度和预后的生物标志物。在这种背景下,一些血清和/或脑脊液生物标志物正在出现,可能在临床实践中用于诊断和治疗目的。这些包括抗体滴度、细胞因子谱、补体因子以及神经元(如神经丝轻链)或星形胶质细胞(如胶质纤维酸性蛋白)损伤标志物。本综述的目的是总结关于新兴诊断和预后生物标志物在NMOSD和MOGAD患者中作用的当前证据。