Department of Clinical Science, Bergen Integrated Diagnostic Stewardship Cluster, Faculty of Medicine, University of Bergen, Bergen, Norway.
Department of Microbiology, Haukeland University Hospital, University of Bergen, Bergen, Norway.
Front Immunol. 2022 Mar 17;13:801616. doi: 10.3389/fimmu.2022.801616. eCollection 2022.
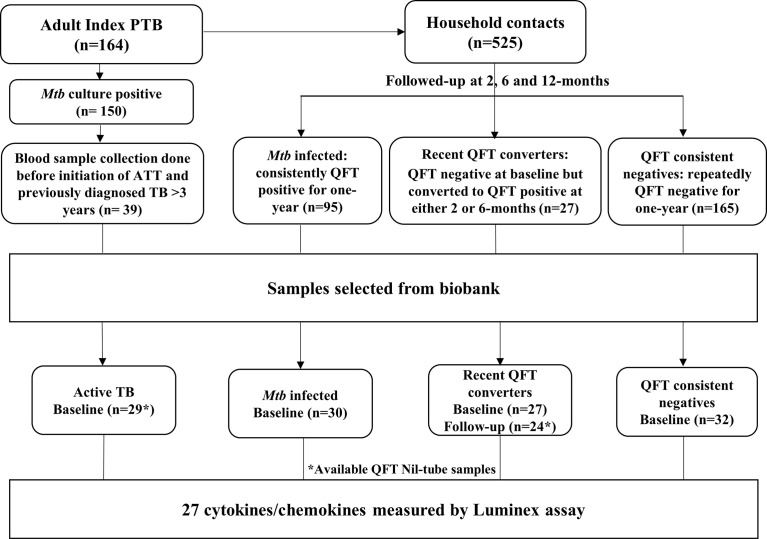
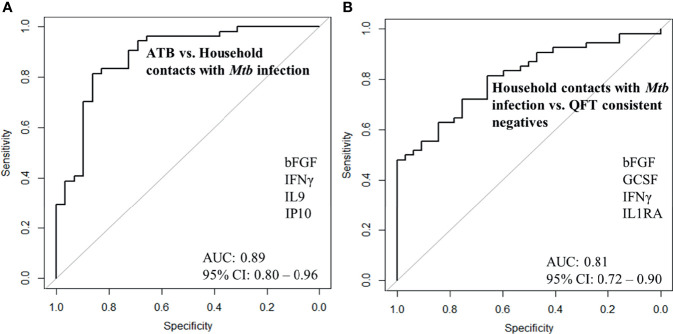
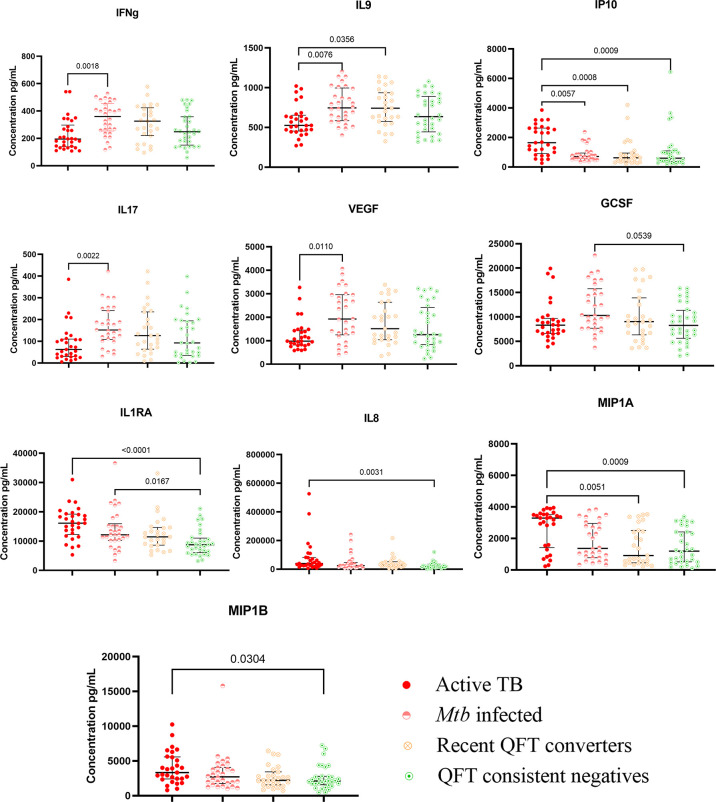
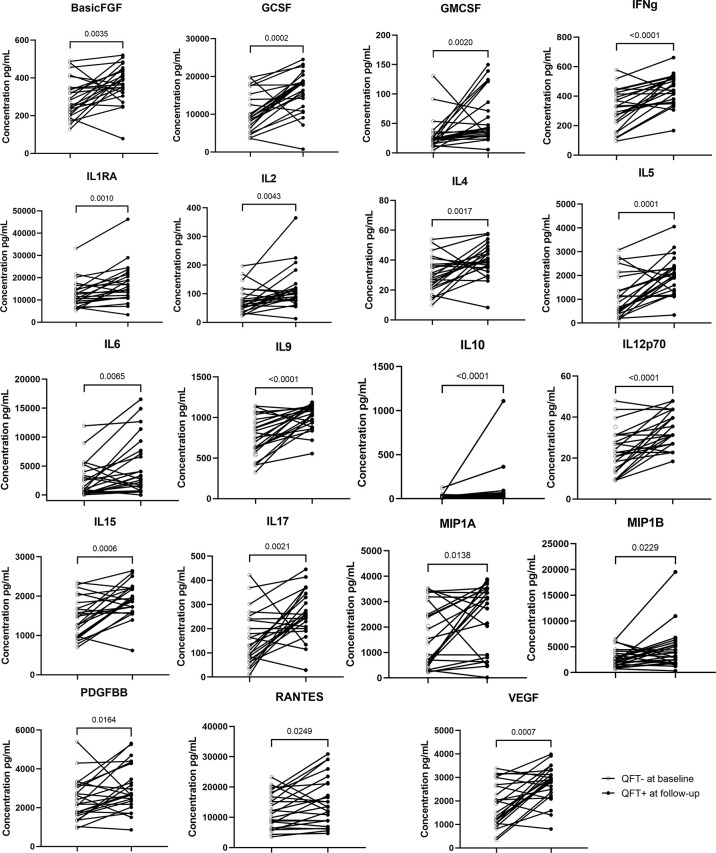
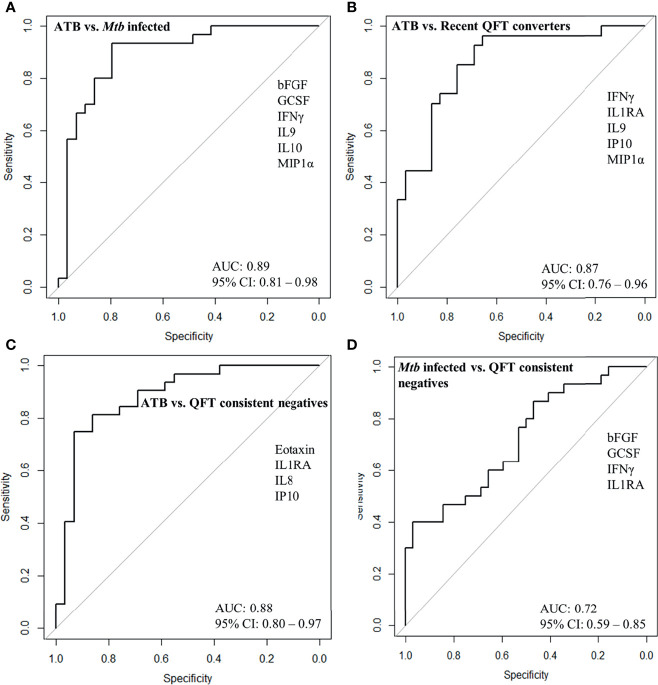
Delays in diagnosis and treatment of pulmonary tuberculosis (TB) can lead to more severe disease and increased transmission. Contact investigation among household contacts (HHCs) of TB patients is crucial to ensure optimal outcomes. In the context of a prospective cohort study in Palamaner, Southern India, this study attempted to assess the potential of 27 different soluble immune markers to accurately assign HHCs for appropriate treatment. A multiplex bead assay was applied on QuantiFERON (QFT)-nil supernatants collected from 89 HHCs grouped by longitudinal QFT status; () infected (QFT positive at baseline and follow-up, n = 30), recent QFT converters (QFT-negative at baseline, n = 27) and converted to QFT-positivity within 6 months of exposure (at follow-up, n = 24) and QFT consistent negatives (n = 32). The 29 TB index cases represented Active TB. Active TB cases and HHCs with infection produced significantly different levels of both pro-inflammatory (IFNγ, IL17, IL8, IP10, MIP-1α, MIP1β, and VEGF) and anti-inflammatory (IL9 and IL1RA) cytokines. We identified a 4-protein signature (bFGF, IFNγ, IL9, and IP10) that correctly classified HHCs with infection vs. Active TB with a specificity of 92.6%, suggesting that this 4-protein signature has the potential to assign HHCs for either full-length TB treatment or preventive TB treatment. We further identified a 4-protein signature (bFGF, GCSF, IFNγ, and IL1RA) that differentiated HHCs with infection from QFT consistent negatives with a specificity of 62.5%, but not satisfactory to safely assign HHCs to no preventive TB treatment. QFT conversion, reflecting new infection, induced an elevated median concentration in nearly two-thirds (19/27) of the analyzed soluble markers compared to the levels measured at baseline. Validation in other studies is warranted in order to establish the potential of the immune biosignatures for optimized TB case detection and assignment to therapeutic and preventive treatment of infected individuals.
肺结核(TB)的诊断和治疗延误可导致病情加重和传播增加。对 TB 患者的家庭接触者(HHC)进行接触调查对于确保最佳结果至关重要。在印度南部 Palamaner 的一项前瞻性队列研究中,本研究试图评估 27 种不同可溶性免疫标志物的潜力,以准确分配 HHC 进行适当的治疗。应用多重珠粒分析(bead assay)对来自 89 名 HHC 的 QuantiFERON(QFT)-nil 上清液进行检测,这些 HHC 按纵向 QFT 状态分组;()感染(基线和随访时 QFT 阳性,n=30)、近期 QFT 转化者(基线时 QFT 阴性,n=27)和在接触后 6 个月内转化为 QFT 阳性(随访时,n=24)和 QFT 持续阴性(n=32)。29 例 TB 索引病例代表活动性 TB。活动性 TB 病例和感染的 HHC 产生的促炎(IFNγ、IL17、IL8、IP10、MIP-1α、MIP1β 和 VEGF)和抗炎(IL9 和 IL1RA)细胞因子水平明显不同。我们确定了一个 4 蛋白特征(bFGF、IFNγ、IL9 和 IP10),可以正确分类感染的 HHC 与活动性 TB,特异性为 92.6%,这表明该 4 蛋白特征有可能将 HHC 分配给全疗程 TB 治疗或预防性 TB 治疗。我们还确定了一个 4 蛋白特征(bFGF、GCSF、IFNγ 和 IL1RA),可以将感染的 HHC 与 QFT 持续阴性区分开来,特异性为 62.5%,但不足以安全地将 HHC 分配给无预防性 TB 治疗。QFT 转化,反映了新的感染,与基线测量的水平相比,在近三分之二(19/27)分析的可溶性标志物中诱导了中位数浓度升高。需要在其他研究中进行验证,以确定免疫生物标志物在优化 TB 病例检测和分配给感染个体的治疗和预防性治疗方面的潜力。