Jung Seung Jin, Kim Bum Joon, Kim Chi Kyung, Shim Sung Ryul, Jung Jin-Man
Department of Neurology, Korea University College of Medicine, Seoul, Republic of Korea.
Department of Family Medicine, Gimpo Woori Hospital, Gimpo, Republic of Korea.
Ann Transl Med. 2022 Mar;10(5):245. doi: 10.21037/atm-21-3748.
It is still uncertain which antiplatelet regimen had the greatest net clinical benefit in patients who have suffered a transient ischemic attack or non-cardioembolic ischemic stroke, and it is necessary to choose the optimal regimen according to the clinical situation.
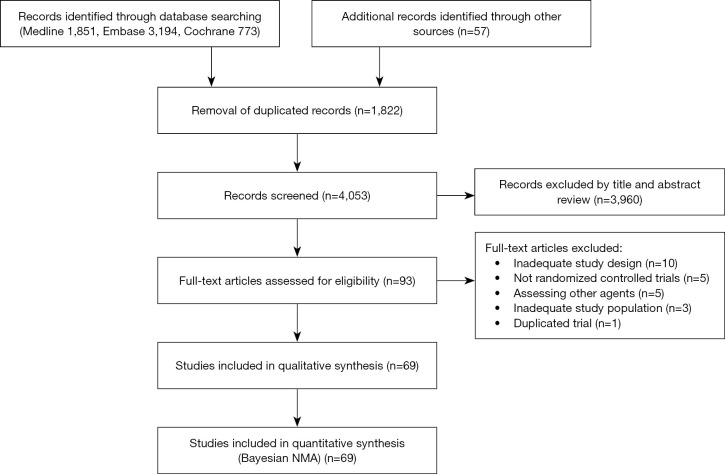
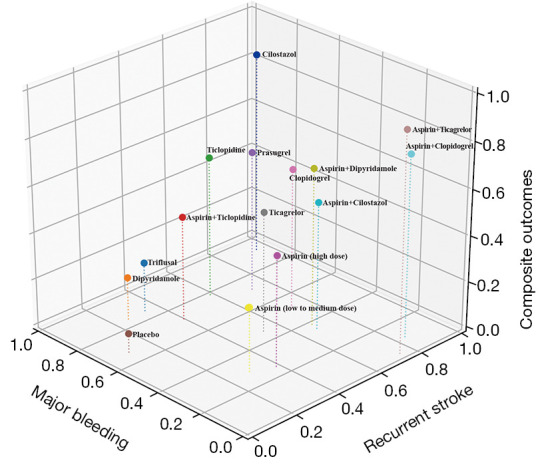
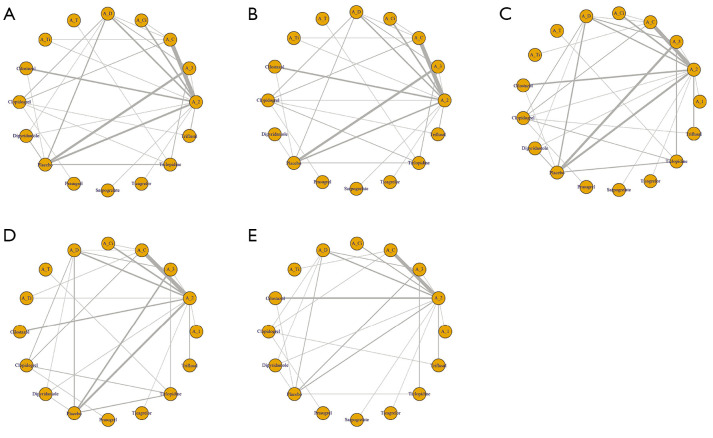
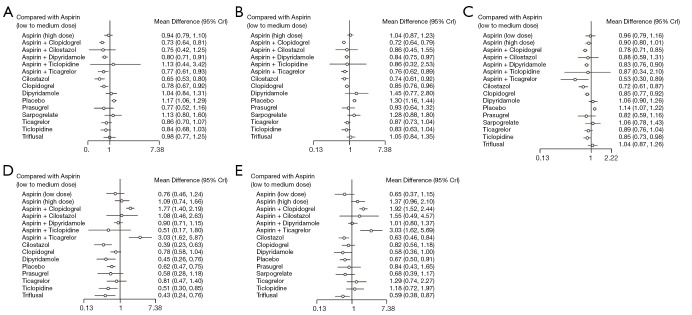
We utilized 3 databases of Medline, Embase, and the Cochrane Central Register of Controlled Trials to find randomized controlled trials that met our criteria, and performed network meta-analyses in recurrent stroke, composite outcomes, major bleeding events, recurrent ischemic stroke, and all bleeding events. Three-dimensional clustered rank plots were used to obtain the net clinical benefit. Subgroup analyses were performed according to the symptom-onset-to-treatment time (<72 and >72 h), stroke subtypes (large artery atherosclerosis and small vessel occlusion), and dual antiplatelet agent treatment duration.
A total of 69 trials were enrolled. Cilostazol was associated with a lower risk of recurrent stroke, major bleeding events, composite outcomes, recurrent ischemic stroke, and all bleeding events compared to low to medium dose aspirin. The three-dimensional rank plot showed that cilostazol had the highest net clinical benefit. The combination of aspirin plus clopidogrel had greater efficacy in the <72 h after stroke onset and large artery atherosclerosis subgroups, and when it was restricted to1 month of use major bleeding risk was not higher than aspirin. The combination of aspirin plus dipyridamole had greater efficacy and safety comparable to aspirin in terms of small vessel occlusion.
The efficacy and safety profiles among antiplatelet regimens may differ according to clinical situation, although cilostazol, aspirin plus clopidogrel, and aspirin plus dipyridamole may be considered as preferable options.
对于短暂性脑缺血发作或非心源性缺血性卒中患者,哪种抗血小板治疗方案具有最大的净临床获益仍不明确,有必要根据临床情况选择最佳方案。
我们利用Medline、Embase和Cochrane对照试验中央注册库这3个数据库查找符合我们标准的随机对照试验,并对复发性卒中、复合结局、大出血事件、复发性缺血性卒中和所有出血事件进行网状Meta分析。使用三维聚类秩和图来获得净临床获益。根据症状发作至治疗时间(<72小时和>72小时)、卒中亚型(大动脉粥样硬化和小血管闭塞)以及双联抗血小板药物治疗持续时间进行亚组分析。
共纳入69项试验。与低至中剂量阿司匹林相比,西洛他唑与复发性卒中、大出血事件、复合结局、复发性缺血性卒中和所有出血事件的风险较低相关。三维秩和图显示西洛他唑具有最高的净临床获益。阿司匹林加氯吡格雷的联合用药在卒中发作后<72小时和大动脉粥样硬化亚组中疗效更佳,且当限制使用1个月时,大出血风险不高于阿司匹林。阿司匹林加双嘧达莫的联合用药在小血管闭塞方面的疗效和安全性与阿司匹林相当。
抗血小板治疗方案的疗效和安全性可能因临床情况而异,尽管西洛他唑、阿司匹林加氯吡格雷以及阿司匹林加双嘧达莫可能被视为更优选择。