Kim Hyeun-Sung, Wu Pang-Hung, Grasso Giovanni, An Jin-Woo, Kim Myeonghun, Lee Inkyung, Park Jong-Seon, Lee Jun-Hyoung, Kang Sangsoo, Lee Jeongshik, Yi Yeonjin, Lee Jun-Hyung, Park Jun-Hwan, Lim Jae-Hyeon, Jang Il-Tae
Spine Surgery, Nanoori Gangnam Hospital, Seoul 06048, Korea.
Department of Orthopaedic Surgery, Juronghealth Campus, National University Health System, Singapore 609606, Singapore.
Diagnostics (Basel). 2022 Mar 24;12(4):793. doi: 10.3390/diagnostics12040793.
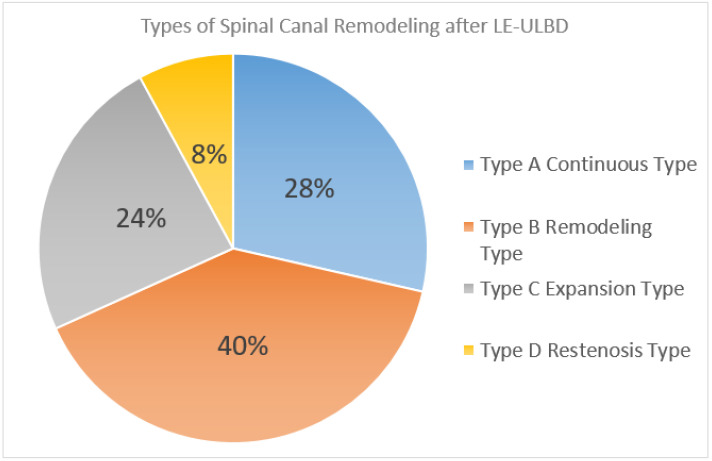
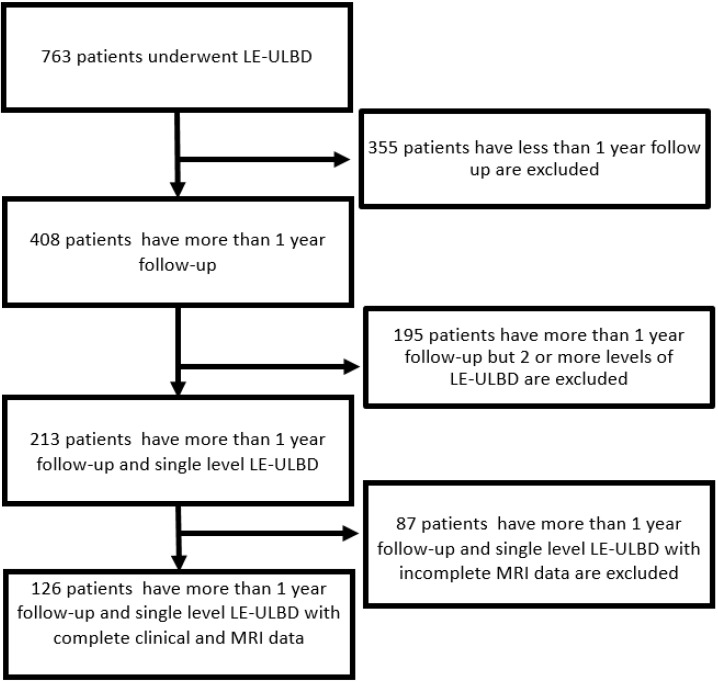
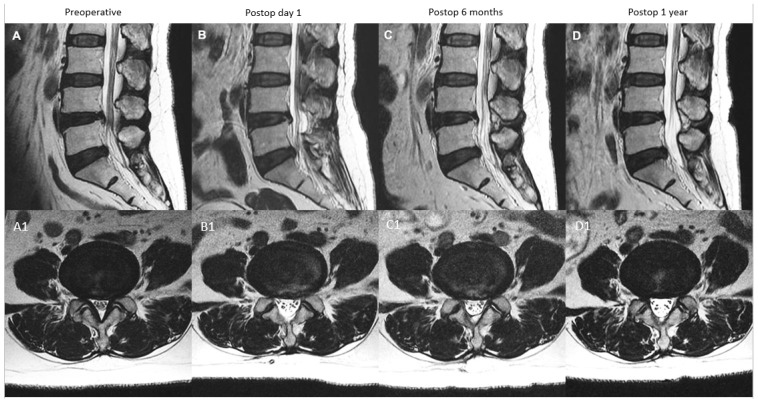
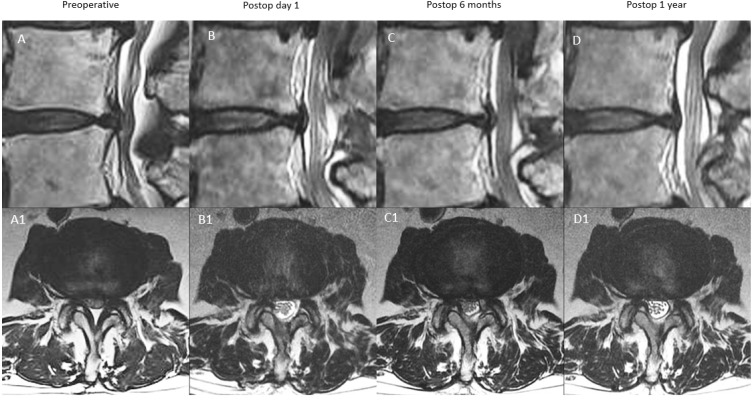
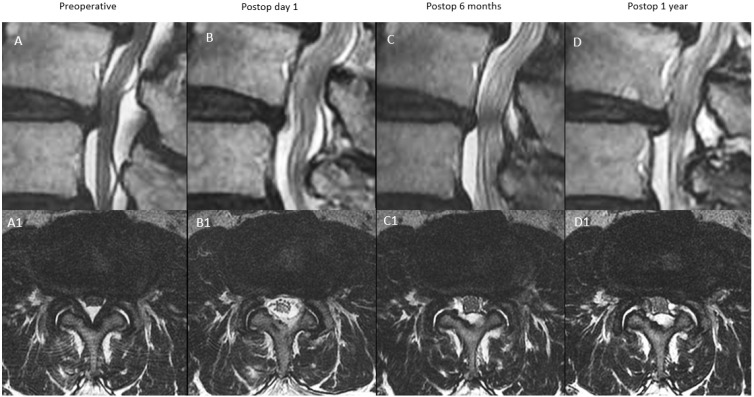
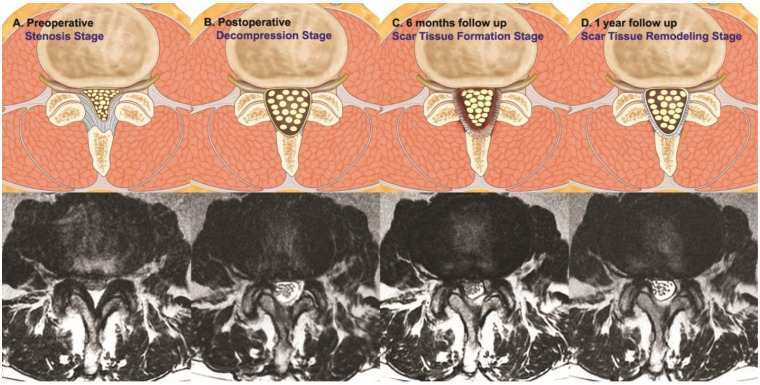
Objective: There is limited literature on repetitive postoperative MRI and clinical evaluation after Uniportal Lumbar Endoscopic Unilateral Laminotomy for Bilateral Decompression. Methods: Clinical visual analog scale, Oswestry Disability Index, McNab’s criteria evaluation and MRI evaluation of the axial cut spinal canal area of the upper end plate, mid disc and lower end plate were performed for patients who underwent single-level Uniportal Lumbar Endoscopic Unilateral Laminotomy for Bilateral Decompression. From the evaluation of the axial cut MRI, four types of patterns of remodeling were identified: type A: continuous expanded spinal canal, type B: restenosis with delayed expansion, type C: progressive expansion and type D: restenosis. Result: A total of 126 patients with single-level Uniportal Lumbar Endoscopic Unilateral Laminotomy for Bilateral Decompression were recruited with a minimum follow-up of 26 months. Thirty-six type A, fifty type B, thirty type C and ten type D patterns of spinal canal remodeling were observed. All four types of patterns of remodeling had statistically significant improvement in VAS at final follow-up compared to the preoperative state with type A (5.59 ± 1.58), B (5.58 ± 1.71), C (5.58 ± 1.71) and D (5.27 ± 1.68), p < 0.05. ODI was significantly improved at final follow-up with type A (49.19 ± 10.51), B (50.00 ± 11.29), C (45.60 ± 10.58) and D (45.60 ± 10.58), p < 0.05. A significant MRI axial cut increment of the spinal canal area was found at the upper endplate at postoperative day one and one year with type A (39.16 ± 22.73; 28.00 ± 42.57) mm2, B (47.42 ± 18.77; 42.38 ± 19.29) mm2, C (51.45 ± 18.16; 49.49 ± 18.41) mm2 and D (49.10 ± 23.05; 38.18 ± 18.94) mm2, respectively, p < 0.05. Similar significant increment was found at the mid-disc at postoperative day one, 6 months and one year with type A (55.16 ± 27.51; 37.23 ± 25.88; 44.86 ± 25.73) mm2, B (72.83 ± 23.87; 49.79 ± 21.93; 62.94 ± 24.43) mm2, C (66.85 ± 34.48; 54.92 ± 30.70; 64.33 ± 31.82) mm2 and D (71.65 ± 16.87; 41.55 ± 12.92; 49.83 ± 13.31) mm2 and the lower endplate at postoperative day one and one year with type A (49.89 ± 34.50; 41.04 ± 28.56) mm2, B (63.63 ± 23.70; 54.72 ± 24.29) mm2, C (58.50 ± 24.27; 55.32 ± 22.49) mm2 and D (81.43 ± 16.81; 58.40 ± 18.05) mm2 at postoperative day one and one year, respectively, p < 0.05. Conclusions: After full endoscopic lumbar decompression, despite achieving sufficient decompression immediately postoperatively, varying severity of asymptomatic restenosis was found in postoperative six months MRI without clinical significance. Further remodeling with a varying degree of increment of the spinal canal area occurs at postoperative one year with overall good clinical outcomes.
关于单孔腰椎内镜下双侧减压单侧椎板切开术后重复进行MRI检查及临床评估的文献有限。方法:对接受单节段单孔腰椎内镜下双侧减压单侧椎板切开术的患者进行临床视觉模拟评分、Oswestry功能障碍指数、McNab标准评估,并对上位终板、椎间盘中部和下位终板的轴位椎管面积进行MRI评估。通过对轴位MRI评估,确定了四种重塑模式:A型:椎管持续扩大;B型:再狭窄伴延迟扩张;C型:进行性扩张;D型:再狭窄。结果:共纳入126例行单节段单孔腰椎内镜下双侧减压单侧椎板切开术的患者,最短随访26个月。观察到36例A型、50例B型、30例C型和10例D型椎管重塑模式。与术前状态相比,所有四种重塑模式在末次随访时VAS均有统计学显著改善,A型(5.59±1.58)、B型(5.58±1.71)、C型(5.58±1.71)和D型(5.27±1.68),p<0.05。末次随访时ODI有显著改善,A型(49.19±10.51)、B型(50.00±11.29)、C型(45.60±10.58)和D型(45.60±10.58),p<0.05。术后第1天和1年,上位终板椎管面积MRI轴位有显著增加,A型分别为(39.16±22.73;28.00±42.57)mm²、B型(47.42±18.77;42.38±19.29)mm²、C型(51.45±18.16;49.49±18.41)mm²和D型(49.10±23.05;38.18±18.94)mm²,p<0.05。术后第1天、6个月和1年,椎间盘中部也有类似的显著增加,A型分别为(55.16±27.51;37.23±25.88;44.86±25.73)mm²、B型(72.83±23.87;49.79±21.93;62.94±24.43)mm²、C型(66.85±34.48;54.92±30.70;64.33±31.82)mm²和D型(71.65±16.87;41.55±12.92;49.83±13.31)mm²;术后第1天和1年,下位终板也有显著增加,A型分别为(49.89±34.50;41.04±28.56)mm²、B型(63.63±23.70;54.72±24.29)mm²、C型(58.50±24.27;55.32±22.49)mm²和D型(81.43±16.81;58.40±18.05)mm²,p<0.05。结论:全内镜下腰椎减压术后,尽管术后立即实现了充分减压,但在术后6个月的MRI中发现了不同程度的无症状再狭窄,无临床意义。术后1年椎管面积有不同程度的进一步重塑增加,总体临床效果良好。