Masiliūnas Rytis, Vilionskis Aleksandras, Bornstein Natan M, Rastenytė Daiva, Jatužis Dalius
Center of Neurology, Vilnius University, Vilnius, Lithuania.
Clinic of Neurology and Neurosurgery, Institute of Clinical Medicine, Faculty of Medicine, Vilnius University, Vilnius, Lithuania.
Eur Stroke J. 2022 Jun;7(2):134-142. doi: 10.1177/23969873221089158. Epub 2022 Apr 7.
Reperfusion therapy (RT) is a mainstay treatment for acute ischemic stroke (AIS). We aimed to evaluate the impact of a comprehensive national policy (CNP) to improve access to RT for AIS patients across Lithuania.
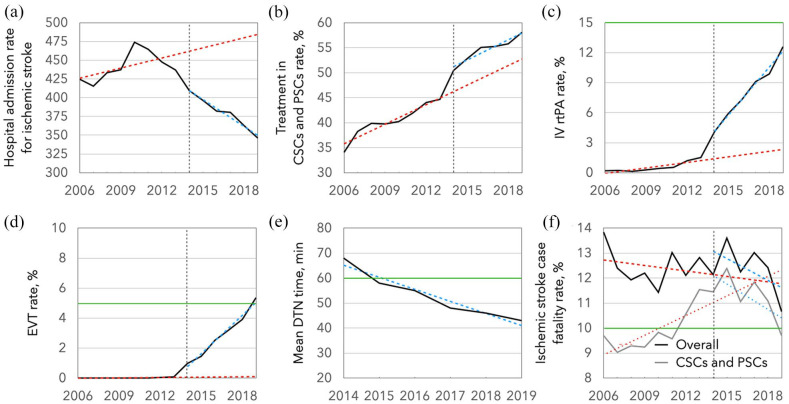
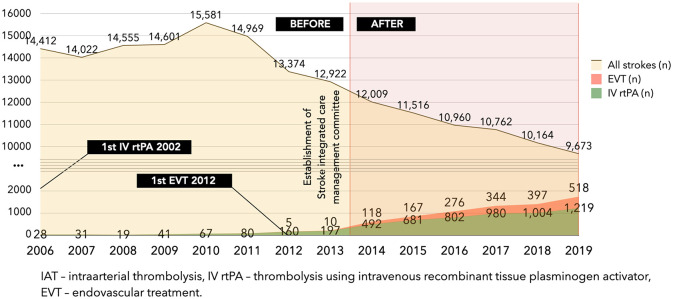
Aggregated anonymized data on AIS cases treated in Lithuanian hospitals between 2006 and 2019 were retrospectively obtained from the Institute of Hygiene and the Stroke Integrated Care Management Committee. Through an interrupted time series analysis, we examined the trends in AIS hospital admissions, RT, and in-hospital case fatality rates prior to the enactment of CNP in 2014, changes immediately after the intervention, and differences in trends between the pre- and post-intervention periods. Mean yearly door-to-needle times were calculated post-intervention.
114,436 cases were treated for AIS in Lithuanian hospitals before, and 65,084 after the government intervention. We observed a significant decreasing post-intervention trend change in AIS hospital admission rate per 100,000 population (regression coefficient ± standard error: β = -16.47 ± 3.95, = 0.002) and an increasing trend change in the proportion of AIS patients who received reperfusion treatment: intravenous thrombolysis (β = 1.42 ± 0.96, < 0.001) and endovascular therapy (β = 0.85 ± 0.05, < 0.001). The proportion of patients treated in stroke centers increased immediately after the intervention (β = 4.95 ± 1.14, = 0.001), but the long-term post-intervention trend did not change. In addition, there was a significant decreasing trend in all cause in-hospital case fatality rate within primary and comprehensive stroke centers after the intervention (β = -0.60 ± 0.18, = 0.008) despite its prompt initial immediate increase (β = 1.68 ± 0.73, = 0.043). The mean countrywide door-to-needle time decreased from 68 min in 2014 to 43 min in 2019.
The comprehensive national stroke patient care policy could be associated with an immediate increase in stroke center treatment rate, increased access to RT, and improved stroke care performance measures.
再灌注治疗(RT)是急性缺血性卒中(AIS)的主要治疗方法。我们旨在评估一项全面的国家政策(CNP)对改善立陶宛AIS患者获得RT治疗的影响。
回顾性地从立陶宛卫生研究所和卒中综合护理管理委员会获取了2006年至2019年期间立陶宛医院治疗的AIS病例的汇总匿名数据。通过中断时间序列分析,我们研究了2014年CNP颁布前AIS住院人数、RT治疗情况及院内病死率的趋势,干预后立即出现的变化,以及干预前后趋势的差异。干预后计算了平均每年的门到针时间。
在政府干预前,立陶宛医院治疗了114436例AIS病例,干预后为65084例。我们观察到,每10万人口中AIS住院率在干预后有显著下降趋势(回归系数±标准误差:β = -16.47 ± 3.95,P = 0.002),接受再灌注治疗的AIS患者比例呈上升趋势:静脉溶栓(β = 1.42 ± 0.96,P < 0.001)和血管内治疗(β = 0.85 ± 0.05,P < 0.001)。干预后,在卒中中心接受治疗的患者比例立即增加(β = 4.95 ± 1.14,P = 0.001),但干预后的长期趋势没有变化。此外,尽管最初立即出现上升(β = 1.68 ± 0.73,P = 0.043),但干预后初级和综合卒中中心所有原因导致的院内病死率有显著下降趋势(β = -0.60 ± 0.18,P = 0.008)。全国范围内的平均门到针时间从2014年的68分钟降至2019年的43分钟。
全面的国家卒中患者护理政策可能与卒中中心治疗率立即提高、获得RT治疗的机会增加以及卒中护理绩效指标改善有关。