Family Medicine and Population Health (FAMPOP), Faculty of Medicine and Health Sciences, University of Antwerp, Antwerp, Belgium.
DSI-NRF Centre of Excellence for Biomedical Tuberculosis Research, SAMRC Centre for Tuberculosis Research, Division of Molecular Biology and Human Genetics, Stellenbosch University, Cape Town, South Africa.
Microb Genom. 2022 Apr;8(4). doi: 10.1099/mgen.0.000815.
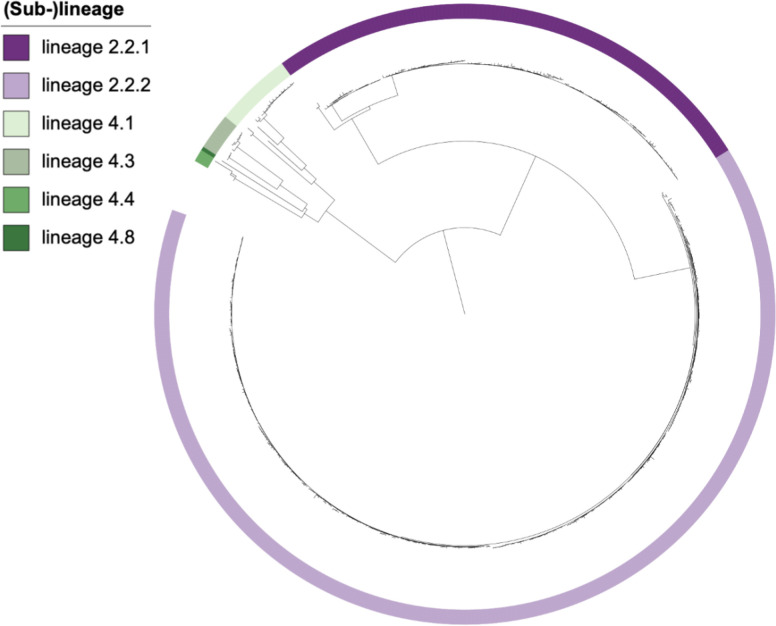
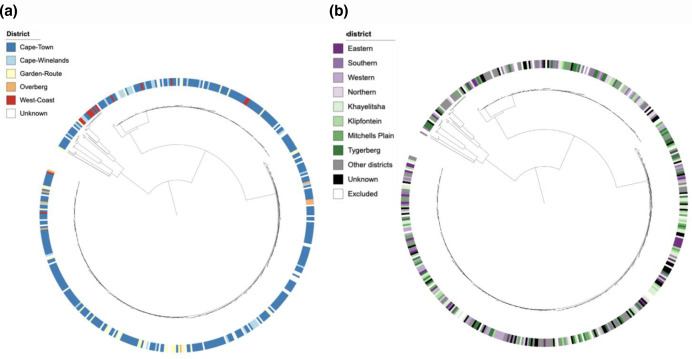
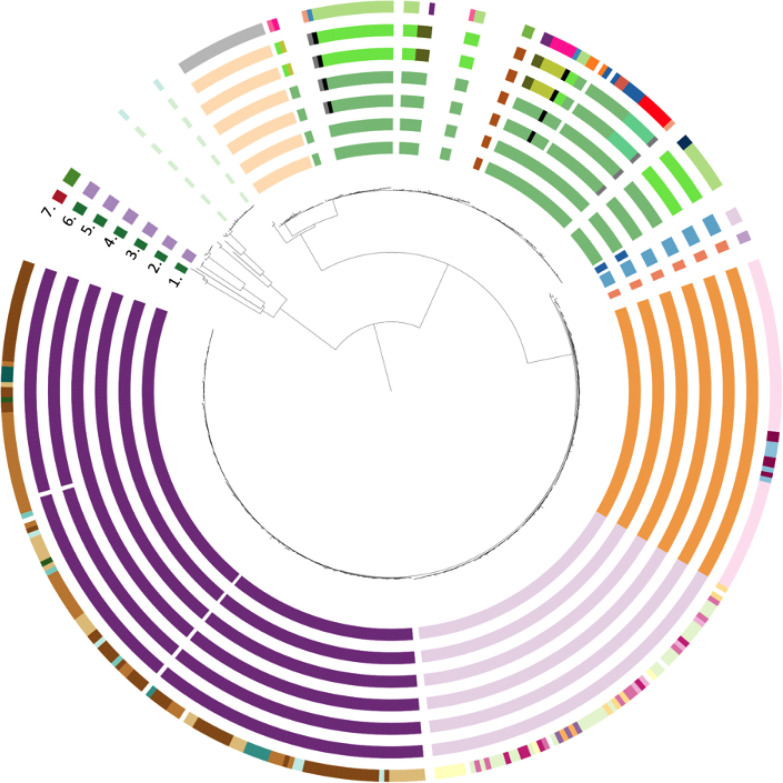
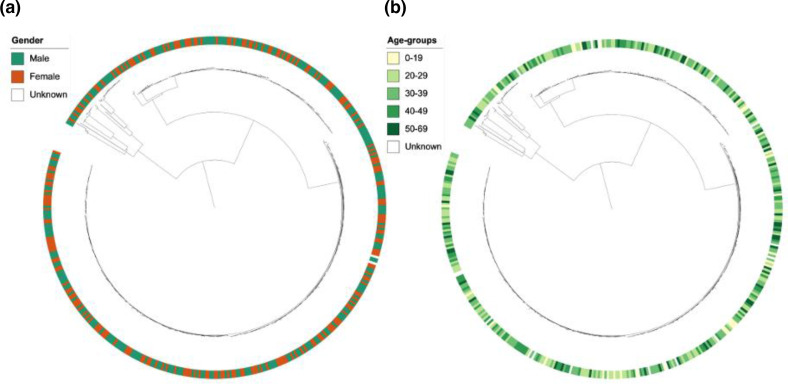
Extensively drug-resistant tuberculosis (XDR-TB), defined as resistance to at least isoniazid (INH), rifampicin (RIF), a fluoroquinolone (FQ) and a second-line injectable drug (SLID), is difficult to treat and poses a major threat to TB control. The transmission dynamics and distribution of XDR () strains have not been thoroughly investigated. Using whole genome sequencing data on 461 XDR- strains, we aimed to investigate the geographical distribution of XDR- strains in the Western Cape Province of South Africa over a 10 year period (2006-2017) and assess the association between sub-lineage, age, gender, geographical patient location and membership or size of XDR-TB clusters. First, we identified transmission clusters by excluding drug resistance-conferring mutations and using the 5 SNP cutoff, followed by merging clusters based on their most recent common ancestor. We then consecutively included variants conferring resistance to INH, RIF, ethambutol (EMB), pyrazinamide (PZA), SLIDs and FQs in the cluster definition. Cluster sizes were classified as small (2-4 isolates), medium (5-20 isolates), large (21-100 isolates) or very large (>100 isolates) to reflect the success of individual strains. We found that most XDR-TB strains were clustered and that including variants conferring resistance to INH, RIF, EMB, PZA and SLIDs in the cluster definition did not significantly reduce the proportion of clustered isolates (85.5-82.2 %) but increased the number of patients belonging to small clusters (4.3-12.4 %, =0.56). Inclusion of FQ resistance-conferring variants had the greatest effect, with 11 clustered isolates reclassified as unique while the number of clusters increased from 17 to 37. Lineage 2 strains (lineage 2.2.1 typical Beijing or lineage 2.2.2 atypical Beijing) showed the large clusters which were spread across all health districts of the Western Cape Province. We identified a significant association between residence in the Cape Town metropole and cluster membership (=0.016) but no association between gender, age and cluster membership or cluster size (=0.39). Our data suggest that the XDR-TB epidemic in South Africa probably has its origin in the endemic spread of MDR and pre-XDR strains followed by acquisition of FQ resistance, with more limited transmission of XDR strains. This only became apparent with the inclusion of drug resistance-conferring variants in the definition of a cluster. In addition to the prevention of amplification of resistance, rapid diagnosis of MDR, pre-XDR and XDR-TB and timely initiation of appropriate treatment is needed to reduce transmission of difficult-to-treat TB.
广泛耐药结核病(XDR-TB)定义为至少对异烟肼(INH)、利福平(RIF)、氟喹诺酮类药物(FQ)和二线注射药物(SLID)耐药,治疗困难,对结核病控制构成重大威胁。XDR 菌株的传播动力学和分布尚未得到彻底调查。我们使用 461 株 XDR 菌株的全基因组测序数据,旨在调查南非西开普省 10 年间(2006-2017 年)XDR 菌株的地理分布,并评估 XDR-TB 簇的亚系、年龄、性别、地理位置、成员或大小之间的关联。首先,我们通过排除耐药相关突变并使用 5 SNP 截止值来识别传播簇,然后根据最近的共同祖先合并簇。然后,我们连续将 INH、RIF、乙胺丁醇(EMB)、吡嗪酰胺(PZA)、SLID 和 FQ 耐药相关变异纳入簇定义中。簇大小分为小(2-4 个分离株)、中(5-20 个分离株)、大(21-100 个分离株)或非常大(>100 个分离株),以反映单个菌株的成功。我们发现大多数 XDR-TB 菌株都聚集在一起,并且将 INH、RIF、EMB、PZA 和 SLID 耐药相关变异纳入簇定义并不会显著降低聚集分离株的比例(85.5-82.2%),但会增加属于小簇的患者数量(4.3-12.4%,=0.56)。纳入 FQ 耐药相关变异的效果最大,有 11 个聚集分离株重新分类为独特分离株,而簇的数量从 17 个增加到 37 个。谱系 2 菌株(谱系 2.2.1 典型北京或谱系 2.2.2 非典型北京)显示出较大的集群,分布在西开普省所有卫生区。我们发现,居住在开普敦大都市与簇成员之间存在显著关联(=0.016),但性别、年龄与簇成员或簇大小之间无关联(=0.39)。我们的数据表明,南非的 XDR-TB 流行可能源于 MDR 和预 XDR 菌株的地方性传播,随后获得 FQ 耐药性,而 XDR 菌株的传播则受到更有限的限制。这只有在簇定义中纳入耐药相关变异时才变得明显。除了防止耐药性扩增外,还需要快速诊断 MDR、预 XDR 和 XDR-TB,并及时开始适当的治疗,以减少难以治疗的结核病的传播。