Division of Environmental and Occupational Health Sciences, National Jewish Health, Denver, CO, USA.
Department of Radiology, National Jewish Health, Denver, CO, USA.
BMC Pulm Med. 2022 Apr 27;22(1):163. doi: 10.1186/s12890-022-01960-w.
Exposure to inhalational hazards during post-9/11 deployment to Southwest Asia and Afghanistan puts military personnel at risk for respiratory symptoms and disease. Pulmonary function and qualitative chest high resolution computed tomography (HRCT) are often normal in "deployers" with persistent respiratory symptoms. We explored the utility of quantitative HRCT imaging markers of large and small airways abnormalities, including airway wall thickness, emphysema, and air trapping, in symptomatic deployers with clinically-confirmed lung disease compared to controls.
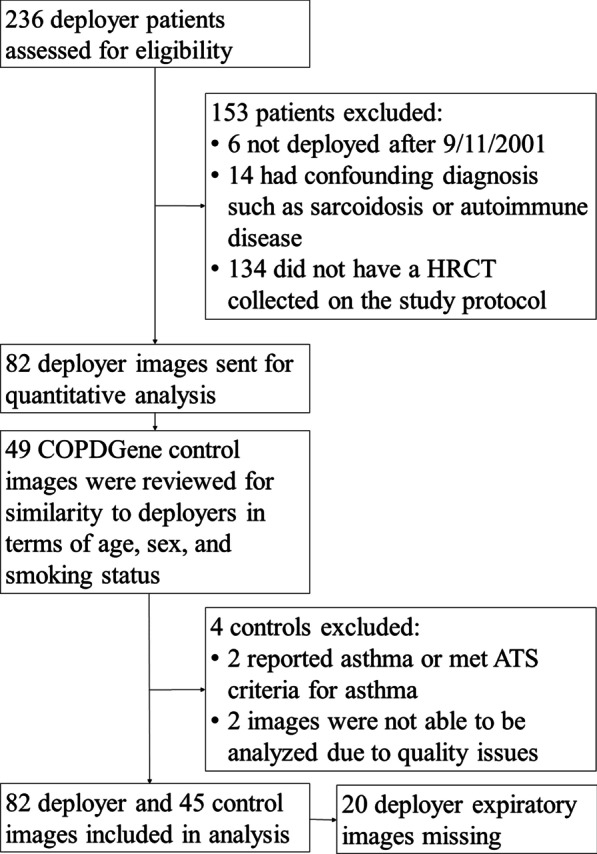
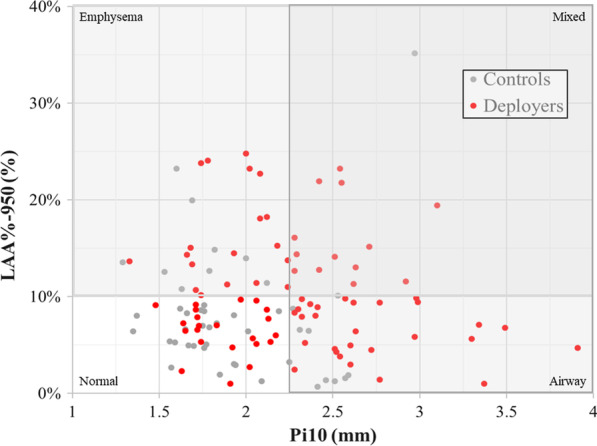
Chest HRCT images from 45 healthy controls and 82 symptomatic deployers with asthma, distal lung disease or both were analyzed using Thirona Lung quantification software to calculate airway wall thickness (by Pi10), emphysema (by percentage of lung volume with attenuation < -950 Hounsfield units [LAA%-950]), and three parameters of air trapping (expiratory/inspiratory total lung volume and mean lung density ratios, and LAA%-856). SAS v.9.4 was used to compare demographic and clinical characteristics between deployers and controls using Chi-Square, Fisher Exact or t-tests. Linear regression was used to assess relationships between pulmonary function and quantitative imaging findings.
Gender and smoking status were not statistically significantly different between groups, but deployers were significantly younger than controls (42 vs 58 years, p < 0.0001), had higher body mass index (31 vs 28 kg/m, p = 0.01), and had fewer total smoking pack-years (8 vs. 26, p = 0.007). Spirometric measures were not statistically significantly different between groups. Pi10 and LAA%-950 were significantly elevated in deployers compared to controls in unadjusted analyses, with the emphysema measure remaining significantly higher in deployers after adjustment for age, sex, smoking, BMI, and expiratory total lung volume. Air trapping parameters were more common in control images, likely due to differences in age and smoking between groups. Among deployers, LAA%-950 and Pi10 were significantly correlated with spirometric markers of obstruction based on ratio of forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) and/or percent predicted FEV1.
Quantitative chest HRCT imaging analysis identifies emphysema in deployers with asthma and distal lung disease, and may be useful in detecting and monitoring deployment-related lung disease in a population where spirometry is typically normal.
在 911 事件后部署到西南亚和阿富汗期间接触吸入性危害,使军人面临呼吸症状和疾病的风险。在持续出现呼吸道症状的“部署者”中,肺功能和定性胸部高分辨率计算机断层扫描(HRCT)通常正常。我们探讨了定量 HRCT 成像大、小气道异常的指标,包括气道壁厚度、肺气肿和空气潴留,在有临床确诊肺部疾病的症状性部署者与对照组中的应用。
使用 Thirona Lung 定量软件分析了 45 名健康对照者和 82 名有哮喘、远端肺部疾病或两者并存的症状性部署者的胸部 HRCT 图像,以计算气道壁厚度(通过 Pi10)、肺气肿(通过衰减值<-950 豪斯菲尔德单位[LAA%-950]的肺体积百分比表示)和空气潴留的三个参数(呼气/吸气总肺容量和平均肺密度比,以及 LAA%-856)。使用 SAS v.9.4 对部署者和对照组之间的人口统计学和临床特征进行比较,使用卡方检验、Fisher 精确检验或 t 检验。使用线性回归评估肺功能与定量成像结果之间的关系。
性别和吸烟状况在组间无统计学差异,但部署者明显比对照组年轻(42 岁 vs. 58 岁,p<0.0001),体重指数较高(31 公斤/米 2 比 28 公斤/米 2 ,p=0.01),吸烟总包年数较少(8 包年 vs. 26 包年,p=0.007)。两组间肺功能指标无统计学差异。在未校正分析中,部署者的 Pi10 和 LAA%-950 明显高于对照组,在调整年龄、性别、吸烟、体重指数和呼气总肺容量后,部署者的肺气肿测量值仍明显较高。在对照组中,空气潴留参数更为常见,这可能是由于组间年龄和吸烟差异所致。在部署者中,LAA%-950 和 Pi10 与基于一秒用力呼气量(FEV1)/用力肺活量(FVC)和/或预计 FEV1 百分比的阻塞性肺功能标志物呈显著相关。
胸部 HRCT 成像定量分析可识别有哮喘和远端肺部疾病的部署者中的肺气肿,并且在肺功能通常正常的人群中,可能有助于检测和监测与部署相关的肺部疾病。