Hou Yue-Min, Yu Hui, Hao Jia-Tao, Feng Fang, An Rui-Fang
Department of Gynecology and Obstetrics, The First Affiliated Hospital of Xi'an Jiaotong University, Xi'an, China.
Front Oncol. 2022 Apr 11;12:860046. doi: 10.3389/fonc.2022.860046. eCollection 2022.
This study aimed to determine the risk and prognostic factors of ovarian cancer (OC) in women having fertility-sparing surgery, as well as survival outcomes of those with stage I epithelial ovarian cancer (EOC). We also determined the effect of chemotherapy in OC treatment and used multiple independent risk factors to establish a prognostic nomogram model for patients with stage I EOC.
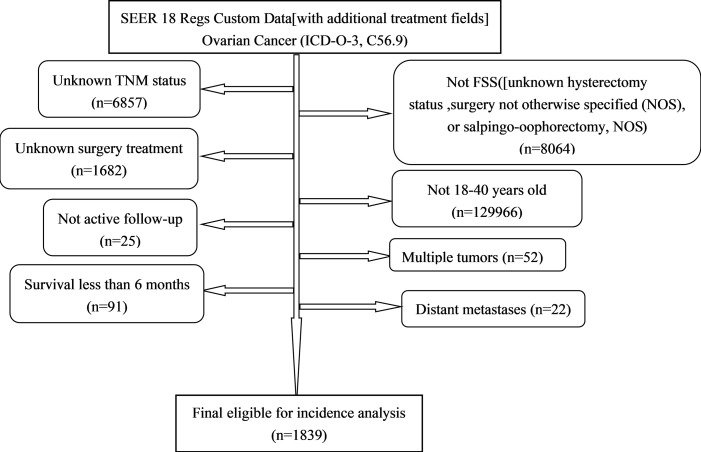
Individuals with OC and with fertility-sparing surgery (FSS) between 1998 and 2016 were identified in the SEER database. Univariate and multivariate logistic regression was performed to identify the distributions of patient characteristics according to chemotherapy. Cancer-specific survival (CSS) was assessed using Kaplan-Meier curves and log-rank tests. Univariate and multivariate Cox regression was conducted to determine the independent prognostic factors for CSS. Cox analysis was used to construct a nomogram model. The C-index and calibration plots showed the performance evaluation results.
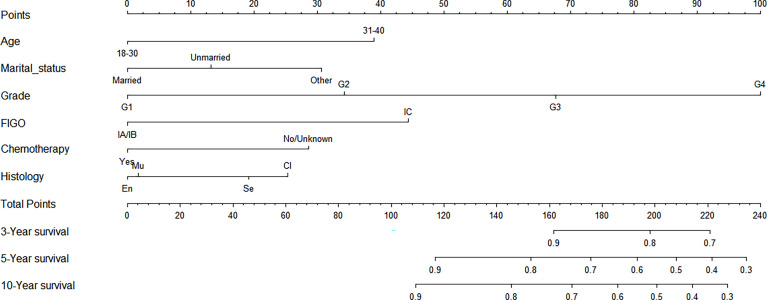
A total of 1,839 women with OC with FSS were identified in the SEER database. Factors associated with significantly higher odds of undergoing chemotherapy included younger age, being unmarried, having grades 2-4, stages II-III, or clear cell and non-epithelial histologic type following a multivariate logistic regression analysis. Multivariate Cox regression analysis confirmed that age, marital status, chemotherapy, histologic type, grade, and the International Federation of Gynecology and Obstetrics (FIGO) stage were independent prognostic factors for CSS. In stage I EOC, the prognosis in patients with stage IA/IB-grade 3 (5-year CSS 85.3%) or stage IC (5-year CSS 80.6%) was worse than that in those with stage IA/IB-grade 1 (5-year CSS 95.2%), or stage IA/IB-grade 2 (5-year CSS 94.7%). However, chemotherapy improved the survival of patients with stage IA/IB-grade 3 (5-year CSS 78.1% vs. 94.6%, = 0.024) or stage IC (5-year CSS 75.1% vs. 86.7%, = 0.170).
The study provided population-based estimates of risk factors and prognoses in patients with OC and with FSS as well as the survival outcomes of patients with stage I EOC and the effect of chemotherapy. The constructed nomograms exhibited superior prognostic discrimination and survival prediction for patients with stage I EOC.
本研究旨在确定接受保留生育功能手术的女性卵巢癌(OC)的风险和预后因素,以及I期上皮性卵巢癌(EOC)患者的生存结局。我们还确定了化疗在OC治疗中的作用,并使用多个独立风险因素为I期EOC患者建立了预后列线图模型。
在监测、流行病学和最终结果(SEER)数据库中识别出1998年至2016年间接受OC治疗并进行保留生育功能手术(FSS)的个体。进行单因素和多因素逻辑回归分析,以确定根据化疗情况的患者特征分布。使用Kaplan-Meier曲线和对数秩检验评估癌症特异性生存(CSS)。进行单因素和多因素Cox回归分析,以确定CSS的独立预后因素。使用Cox分析构建列线图模型。C指数和校准图显示了性能评估结果。
在SEER数据库中总共识别出1839例接受FSS的OC女性患者。多因素逻辑回归分析显示,与接受化疗几率显著更高相关的因素包括年龄较小、未婚、组织学分级为2-4级、II-III期、透明细胞和非上皮组织学类型。多因素Cox回归分析证实,年龄、婚姻状况、化疗、组织学类型、分级以及国际妇产科联盟(FIGO)分期是CSS的独立预后因素。在I期EOC中,IA/IB期3级(5年CSS为85.3%)或IC期(5年CSS为80.6%)患者的预后比IA/IB期1级(5年CSS为95.2%)或IA/IB期2级(5年CSS为94.7%)患者差。然而,化疗改善了IA/IB期3级(5年CSS:78.1%对94.6%,P = 0.024)或IC期(5年CSS:75.1%对86.7%,P = 0.170)患者的生存情况。
本研究提供了基于人群的OC且接受FSS患者的风险因素和预后估计,以及I期EOC患者的生存结局和化疗效果。构建的列线图对I期EOC患者具有卓越的预后判别能力和生存预测能力。