Faculty of Medicine and University Hospital Cologne, Department of Neurology, University of Cologne, Cologne, Germany.
Cognitive Neuroscience, Institute of Neuroscience and Medicine (INM-3), Research Centre Jülich, Jülich, Germany.
Brain. 2023 Mar 1;146(3):1006-1020. doi: 10.1093/brain/awac157.
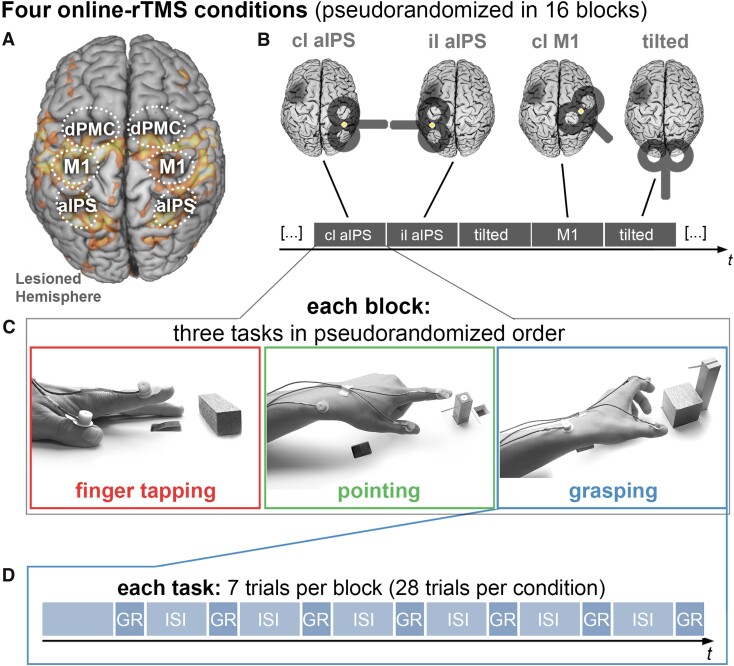
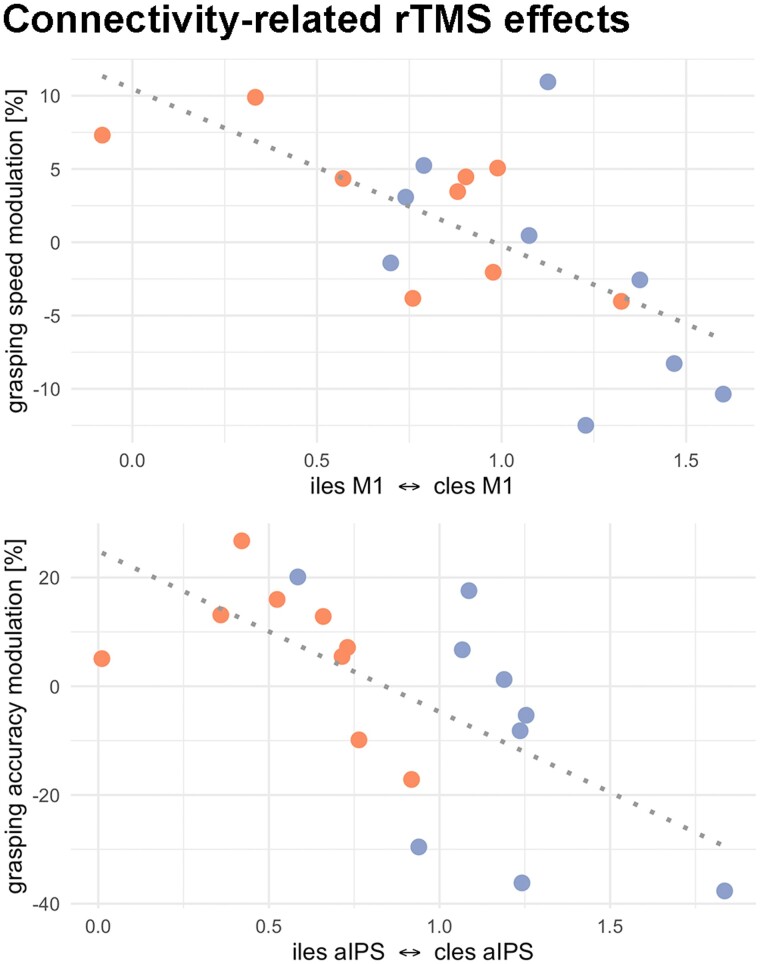
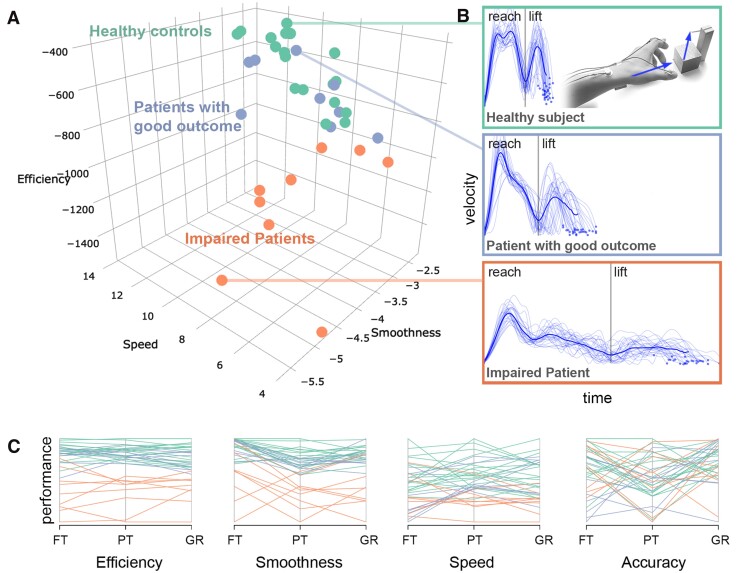
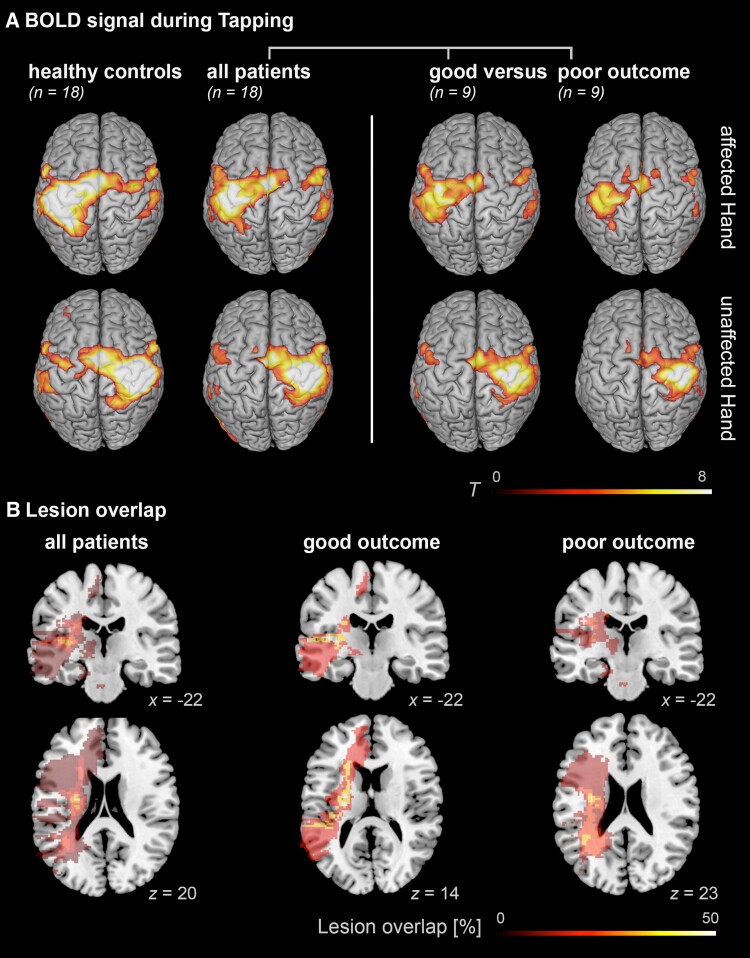
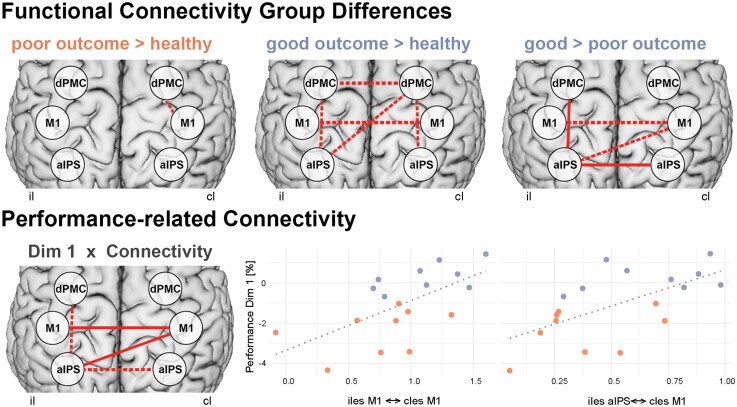
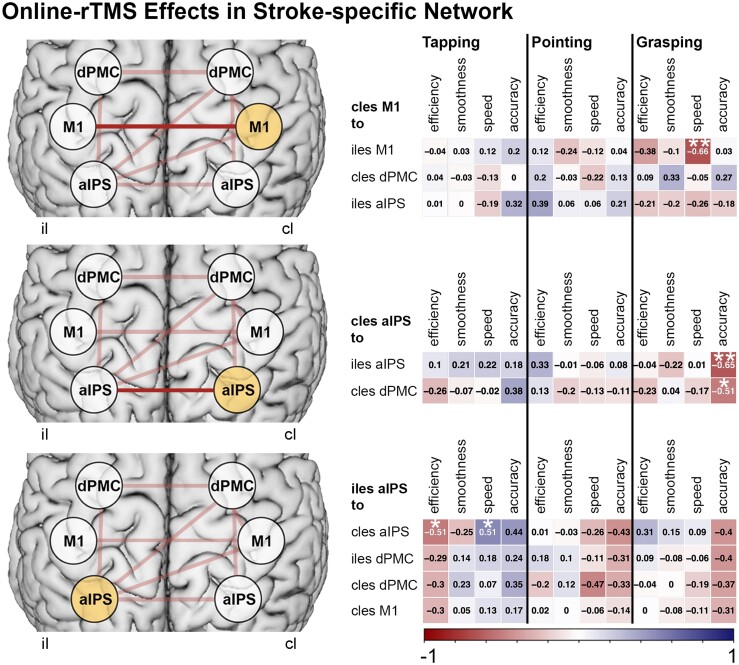
Activity changes in the ipsi- and contralesional parietal cortex and abnormal interhemispheric connectivity between these regions are commonly observed after stroke, however, their significance for motor recovery remains poorly understood. We here assessed the contribution of ipsilesional and contralesional anterior intraparietal cortex (aIPS) for hand motor function in 18 recovered chronic stroke patients and 18 healthy control subjects using a multimodal assessment consisting of resting-state functional MRI, motor task functional MRI, online-repetitive transcranial magnetic stimulation (rTMS) interference, and 3D movement kinematics. Effects were compared against two control stimulation sites, i.e. contralesional M1 and a sham stimulation condition. We found that patients with good motor outcome compared to patients with more substantial residual deficits featured increased resting-state connectivity between ipsilesional aIPS and contralesional aIPS as well as between ipsilesional aIPS and dorsal premotor cortex. Moreover, interhemispheric connectivity between ipsilesional M1 and contralesional M1 as well as ipsilesional aIPS and contralesional M1 correlated with better motor performance across tasks. TMS interference at individual aIPS and M1 coordinates led to differential effects depending on the motor task that was tested, i.e. index finger-tapping, rapid pointing movements, or a reach-grasp-lift task. Interfering with contralesional aIPS deteriorated the accuracy of grasping, especially in patients featuring higher connectivity between ipsi- and contralesional aIPS. In contrast, interference with the contralesional M1 led to impaired grasping speed in patients featuring higher connectivity between bilateral M1. These findings suggest differential roles of contralesional M1 and aIPS for distinct aspects of recovered hand motor function, depending on the reorganization of interhemispheric connectivity.
活动变化在同侧和对侧顶叶皮层和异常的大脑两半球之间的连接这些地区通常观察到后中风,然而,他们的意义运动恢复仍然知之甚少。我们在这里评估同侧和对侧前顶内沟(ipsilesional 和 aIPS)的贡献手电机能在 18 例恢复慢性中风患者和 18 例健康对照组使用一个多模态评估包括静息状态功能磁共振成像、电机任务功能磁共振成像、在线重复经颅磁刺激(rTMS)干扰和 3 d 运动运动学。效果与两个控制刺激部位进行了比较,即对侧 M1 和 sham 刺激条件。我们发现患者运动功能良好的结果相比,患者有更实质性的残留缺陷的特点增加静息状态连接同侧和对侧 aIPS 和同侧 aIPS 和背侧运动前皮层之间。此外,同侧 M1 和对侧 M1之间的大脑两半球之间的连接以及同侧 aIPS 和对侧 M1之间的连接与更好的运动性能任务。TMS 干扰在个体 aIPS 和 M1 坐标导致不同的效果取决于电机任务的测试,即索引 finger-tapping、快速指向运动,或一个达到抓取-lift 任务。干扰对侧 aIPS 恶化抓地力的准确性,特别是在患者具有更高的同侧和对侧 aIPS 之间的连接。相反,干扰对侧 M1 导致受损的抓取速度在患者具有更高的连接双侧 M1。这些发现表明不同的作用对侧 M1 和 aIPS 为恢复手电机能的不同方面,取决于大脑两半球之间的连接的重组。