Cheng Yanwei, Qin Lijie, Chen Long
Department of Emergency, Henan Provincial People's Hospital, People's Hospital of Zhengzhou University, People's Hospital of Henan University, Zhengzhou, China.
Front Oncol. 2022 Apr 13;12:879714. doi: 10.3389/fonc.2022.879714. eCollection 2022.
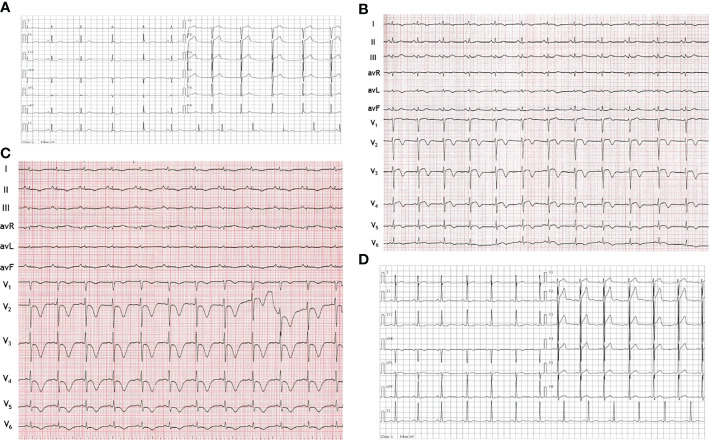
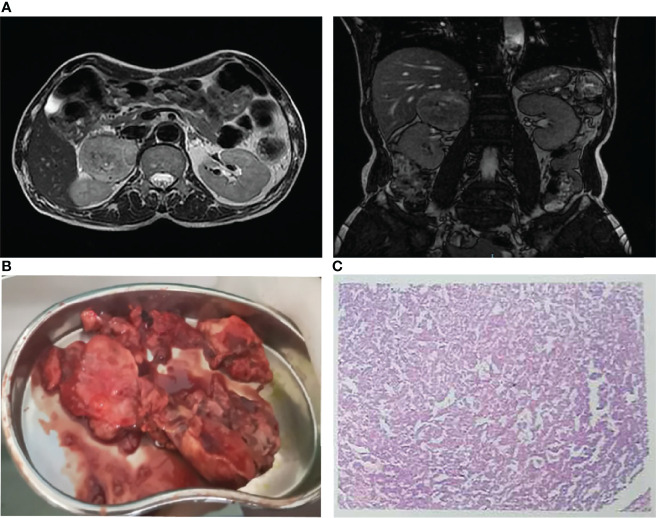
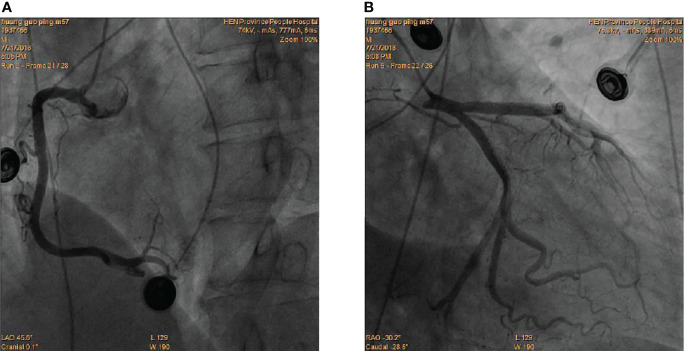
Pheochromocytoma is a rare catecholamine-secreting tumor with highly variable clinical presentations. We herein report a patient who presented to the emergency department with precordia pain, elevated myocardial enzymes, T-wave inversions on electrocardiogram and segmental ventricular wall motion abnormalities on echocardiography, which is normally managed as suspected acute coronary syndrome (ACS). However, the urgent coronary angiography showed normal coronary arteries. During his hospital stay, a sudden increase in blood pressure allowed us to suspect a pheochromocytoma, which was confirmed by elevated levels of catecholamines and by the finding of a right adrenal mass on magnetic resonance imaging. The tumor was successfully excised and the patient is now asymptomatic. This case illustrates that pheochromocytoma can present as a mimic of ACS but this is often difficult to diagnose at first glance and often misleads clinicians into making an incorrect diagnosis. In addition, clinicians should be familiar with clinical manifestations of pheochromocytoma, which can help raise clinical suspicion and facilitate the early diagnosis and treatment of pheochromocytoma.
嗜铬细胞瘤是一种罕见的分泌儿茶酚胺的肿瘤,临床表现高度多变。我们在此报告一名患者,该患者因心前区疼痛、心肌酶升高、心电图T波倒置以及超声心动图显示节段性室壁运动异常而就诊于急诊科,通常这些表现被当作疑似急性冠状动脉综合征(ACS)来处理。然而,紧急冠状动脉造影显示冠状动脉正常。在其住院期间,血压突然升高使我们怀疑患有嗜铬细胞瘤,这一怀疑通过儿茶酚胺水平升高以及磁共振成像发现右侧肾上腺肿块得以证实。肿瘤被成功切除,患者现在无症状。该病例表明,嗜铬细胞瘤可表现为类似ACS,但乍一看往往难以诊断,且常常误导临床医生做出错误诊断。此外,临床医生应熟悉嗜铬细胞瘤的临床表现,这有助于提高临床怀疑并促进嗜铬细胞瘤的早期诊断和治疗。