Department of Public Health, Erasmus MC, University Medical Centre Rotterdam, Rotterdam, The Netherlands.
Ekjut, Chakradharpur, Jharkhand, India.
Int J Equity Health. 2022 May 6;21(1):61. doi: 10.1186/s12939-022-01655-y.
Tribal peoples are among the most marginalised groups worldwide. Evidence on birth outcomes in these groups is scant. We describe inequalities in Stillbirth Rate (SBR), Neonatal Mortality Rate (NMR), and uptake of maternal and newborn health services between tribal and less disadvantaged groups in eastern India, and examine the contribution of poverty and education to these inequalities.
We used data from a demographic surveillance system covering a 1 million population in Jharkhand State (March 2017 - August 2019) to describe SBR, NMR, and service uptake. We used logistic regression analysis combined with Stata's adjrr-command to estimate absolute and relative inequalities by caste/tribe (comparing Particularly Vulnerable Tribal Groups (PVTG) and other Scheduled Tribes (ST) with the less marginalised Other Backward Class (OBC)/none, using the Indian government classification), and by maternal education and household wealth.
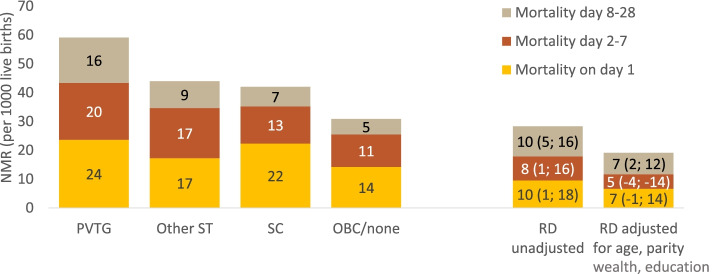
PVTGs had a higher NMR (59/1000) than OBC/none (31/1000) (rate ratio (RR): 1.92, 95%CI: 1.55-2.38). This was partly explained by wealth and education, but inequalities remained large after adjustment (adjusted RR: 1.59, 95%CI: 1.28-1.98). NMR was also higher among other STs (44/1000), but disparities were smaller (RR: 1.47, 95%CI: 1.23-1.75). There was a systematic gradient in NMR by maternal education and household wealth. SBRs were only higher in poorer groups (RR:1.56, 95%CI: 1.14-2.13). Uptake of facility-based services was low among PVTGs (e.g. institutional birth: 25% vs. 69% in OBC/none) and among poorer and less educated women. However, 65% of PVTG women with an institutional birth used a maternity vehicle vs. 34% among OBC/none. Visits from frontline workers (Accredited Social Health Activists [ASHAs]) were similar across groups, and ASHA accompaniment of institutional births was similar across caste/tribe groups, and higher among poorer and less educated women. Attendance in participatory women's groups was similar across caste/tribe groups, and somewhat higher among richer and better educated women.
PVTGs are highly disadvantaged in terms of birth outcomes. Targeted interventions that reduce geographical barriers to facility-based care and address root causes of high poverty and low education in PVTGs are a priority. For population-level impact, they are to be combined with broader policies to reduce socio-economic mortality inequalities. Community-based interventions reach disadvantaged groups and have potential to reduce the mortality gap.
部落民族是世界上最边缘化的群体之一。关于这些群体的出生结局的证据很少。我们描述了在印度东部,部落民族和弱势群体之间的死产率(Stillbirth Rate,SBR)、新生儿死亡率(Neonatal Mortality Rate,NMR)以及母婴健康服务利用率的不平等,并探讨了贫困和教育对这些不平等的贡献。
我们使用了一个人口监测系统的数据,该系统覆盖了印度恰尔康得邦(2017 年 3 月至 2019 年 8 月)的 100 万人口,用于描述 SBR、NMR 和服务利用率。我们使用了逻辑回归分析,并结合 Stata 的 adjrr-命令,根据种姓/部落(将特别脆弱的部落群体( Particularly Vulnerable Tribal Groups,PVTG)和其他在册部落( Other Scheduled Tribes,ST)与较不受影响的其他落后阶层( Other Backward Class,OBC)/无进行比较,使用印度政府的分类)和母亲教育程度和家庭财富来估计绝对和相对不平等。
PVTG 的 NMR(59/1000)高于 OBC/none(31/1000)(比值比(Rate Ratio,RR):1.92,95%置信区间(Confidence Interval,CI):1.55-2.38)。这在一定程度上可以用财富和教育来解释,但调整后仍存在较大差距(调整后的 RR:1.59,95%CI:1.28-1.98)。其他 ST 的 NMR 也较高(44/1000),但差距较小(RR:1.47,95%CI:1.23-1.75)。NMR 也存在系统的梯度,与母亲的教育程度和家庭财富有关。SBR 仅在较贫困的群体中较高(RR:1.56,95%CI:1.14-2.13)。PVTG 中获得基于机构的服务的比例较低(例如,机构分娩:25%与 OBC/none 的 69%),而在较贫困和教育程度较低的妇女中更低。然而,65%的在机构分娩的 PVTG 妇女使用了产妇交通工具,而 OBC/none 的比例为 34%。基层工作者(认证社会卫生活动家(Accredited Social Health Activists,ASHA))的访问在各群体中相似,ASHA 陪同机构分娩的比例在种姓/部落群体中相似,而在较贫困和教育程度较低的妇女中更高。参与妇女参与小组的情况在各群体中相似,而在较富裕和教育程度较高的妇女中略高。
PVTG 在出生结局方面处于高度不利地位。优先考虑针对减少基于机构的护理的地理障碍和解决 PVTG 中贫困和教育程度低的根本原因的针对性干预措施。为了实现人口层面的影响,需要将这些干预措施与更广泛的减少社会经济死亡率不平等的政策相结合。基于社区的干预措施可以覆盖弱势群体,并有可能缩小死亡率差距。