Pérez-Denia Laura, Claffey Paul, Byrne Lisa, Rice Ciara, Kenny Rose Anne, Finucane Ciarán
School of Medicine, Trinity College Dublin, Dublin, Ireland.
Falls and Syncope Unit, Mercer's Institute for Successful Ageing, St. James's Hospital Dublin, Dublin, Ireland.
J Am Geriatr Soc. 2022 Jul;70(7):1973-1986. doi: 10.1111/jgs.17810. Epub 2022 May 10.
Age-related morbidities and frailty are associated with impaired blood pressure (BP) and heart rate (HR) recovery after standing. Here we investigate how multimorbidity affects cerebral and peripheral hemodynamics during standing in a large sample of older patients.
Patients were recruited from a national Falls and Syncope Unit. They underwent an active stand test (5-10 min lying +3 min standing) with monitoring of continuous BP, HR, total peripheral resistance (TPR), stroke volume (SV), and a near-infrared spectroscopy (NIRS) derived cerebral tissue saturation index (TSI). A multimorbidity count was derived from a 26-item list of conditions. Features derived from the signals included: nadir, overshoot, value at 30 s, steady-state and recovery rate. Robust linear regression was used to assess the association between multimorbidity, TSI and peripheral hemodynamics while correcting for covariates. A p-value <0.05 was considered statistically significant.
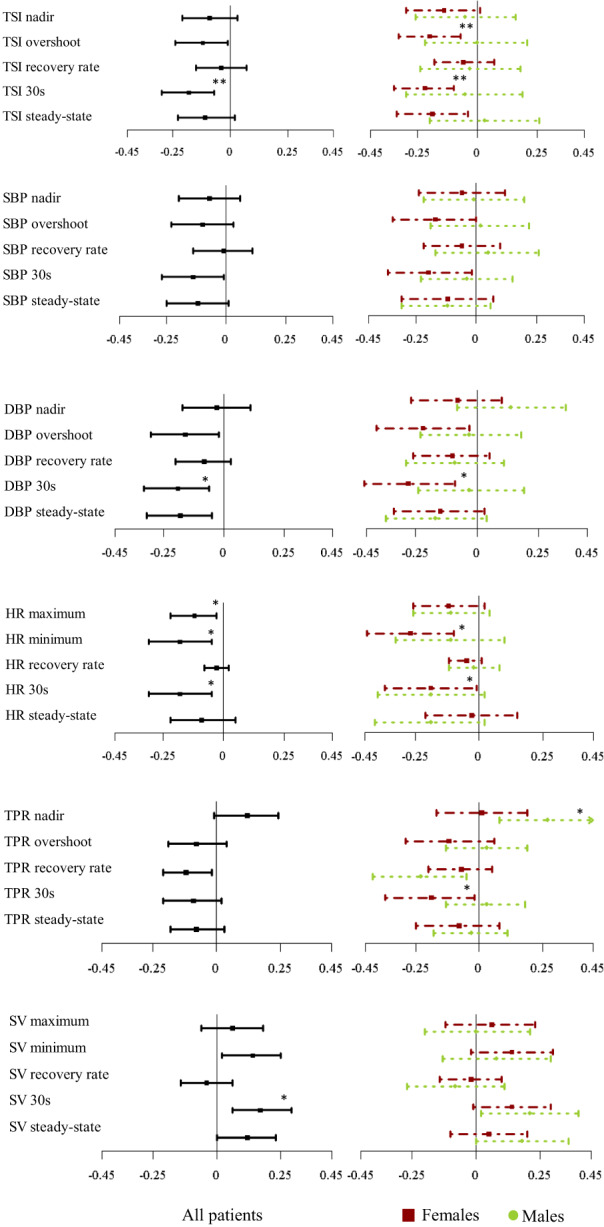
Multimorbidity was associated with poorer recovery of TSI at 30 s after standing (β: -0.15, CI:[-0.25-0.06], p = 0.009) independent of all peripheral hemodynamics. Impaired diastolic BP (DBP) recovery at 30s (β:-1.34, CI:[-2.29-0.40], p = 0.032), DBP steady-state (β:-1.18, CI:[-2.04-0.32], p = 0.032), TPR overshoot-to-nadir difference (β:-0.041, CI:[-0.070-0.013], p = 0.045), and SV at 30s (β:1.30, CI:[0.45 2.15], p = 0.027) were also associated with increasing multimorbidity. After sex stratification, only females demonstrated impaired TSI with multimorbidity at overshoot (β: -0.19, CI: [-0.32 -0.07], p = 0.009), 30 s (β: -0.22 [-0.35-0.10], p = 0.005) and steady-state (β: -0.20, CI:[-0.35-0.04], p = 0.023), independent of peripheral hemodynamics.
Transient cerebral oxygenation and peripheral hemodynamic responses are impaired with multimorbidity (frailty) in older patients, particularly in females. This study demonstrates the feasibility of using NIRS in this clinical context and may inform the development of clinical management strategies targeting both cerebral oxygenation and blood pressure impairments in patients with faints and falls.
与年龄相关的疾病和虚弱与站立后血压(BP)和心率(HR)恢复受损有关。在此,我们研究了多种疾病如何影响大量老年患者站立时的脑和外周血流动力学。
从国家跌倒与晕厥治疗中心招募患者。他们接受了主动站立测试(躺卧5 - 10分钟 + 站立3分钟),同时监测连续血压、心率、总外周阻力(TPR)、每搏输出量(SV)以及通过近红外光谱(NIRS)得出的脑组织氧饱和度指数(TSI)。多种疾病计数来自一份包含26种疾病的清单。从信号中得出的特征包括:最低点、过冲、30秒时的值、稳态和恢复率。在对协变量进行校正的同时,使用稳健线性回归来评估多种疾病、TSI和外周血流动力学之间的关联。p值<0.05被认为具有统计学意义。
多种疾病与站立后30秒时TSI的较差恢复相关(β:-0.15,CI:[-0.25 - 0.06],p = 0.009),且独立于所有外周血流动力学。30秒时舒张压(DBP)恢复受损(β:-1.34,CI:[-2.29 - 0.40],p = 0.032)、DBP稳态(β:-1.18,CI:[-2.04 - 0.32],p = 0.032)、TPR过冲至最低点差值(β:-0.041,CI:[-0.070 - 0.013],p = 0.045)以及30秒时的SV(β:1.30,CI:[0.45 2.15],p = 0.027)也与多种疾病增加相关。按性别分层后,只有女性在过冲(β:-0.19,CI:[-0.32 - 0.07],p = 0.009)、30秒(β:-0.22 [-0.35 - 0.10],p = 0.005)和稳态(β:-0.20,CI:[-0.35 - 0.04],p = 0.023)时表现出多种疾病导致的TSI受损,且独立于外周血流动力学。
老年患者中,多种疾病(虚弱)会损害短暂脑氧合和外周血流动力学反应,尤其是在女性中。本研究证明了在这种临床背景下使用NIRS的可行性,并可能为针对晕厥和跌倒患者的脑氧合和血压损害制定临床管理策略提供依据。