Tella Abhinav, Vang William, Ikeri Eustacia, Taylor Olivia, Zhang Alicia, Mazanec Megan, Raju Srihari, Ishani Areef
Department of Veterans Affairs, Minneapolis Veterans Health Care System, Minneapolis, MN.
Kidney Med. 2022 Apr 1;4(5):100460. doi: 10.1016/j.xkme.2022.100460. eCollection 2022 May.
RATIONALE & OBJECTIVE: There is conflicting evidence regarding the type of β-blockers to use in dialysis patients. This systematic review seeks to determine whether highly dialyzable β-blockers are associated with higher rates of cardiovascular events and mortality in hemodialysis patients than poorly dialyzable β-blockers.
A systematic review of the existing literature was conducted. A meta-analysis was performed using data from the selected studies.
SETTING & STUDY POPULATIONS: Participants were from the United States, Canada, and Taiwan. The mean ages of participants ranged from 55.9-75.7 years.
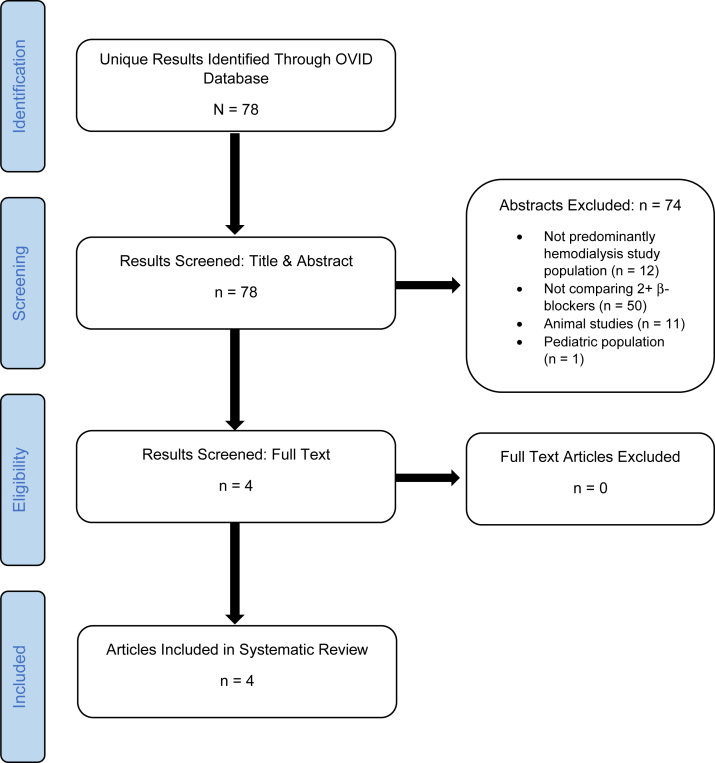
We searched the Ovid MEDLINE database from 1990 to September 2020. Studies without adult hemodialysis participants and without comparisons of at least 2 β-blockers of different dialyzability were excluded.
Baseline and adjusted outcome data were extracted from each study.
Random-effects models were used to calculate pooled risk ratios using fully adjusted models from individual studies.
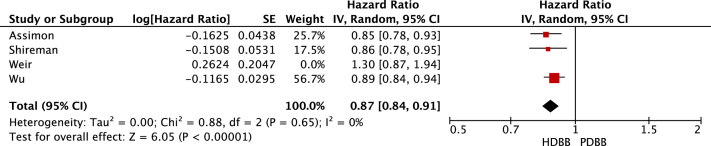
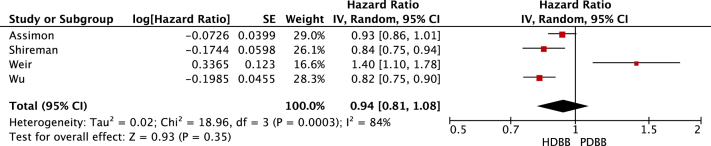
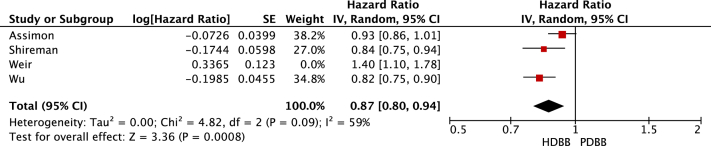
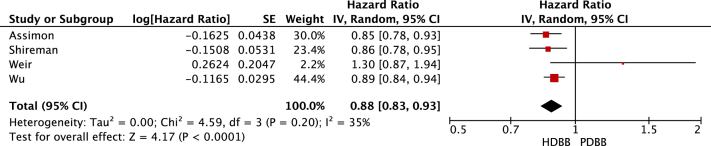
Four cohort studies were included. Pooling fully adjusted models, highly dialyzable β-blockers did not influence mortality (HR, 0.94; 95% CI, 0.81-1.08; I = 0.84) compared with poorly dialyzable β-blockers but were associated with a reduction in cardiovascular events (HR, 0.88; 95% CI, 0.83-0.93). There was significant heterogeneity between studies (I = 0.35). Only 1 study reported on adverse events. Intradialytic hypotension was more common in those on carvedilol (a poorly dialyzable β-blocker) compared with those on metoprolol (a highly dialyzable β-blocker; adjusted incidence rate ratio, 1.10; 95% CI, 1.09-1.11).
No randomized controlled trials were identified. Each study used different analytic methods and different definitions for outcomes. Classifications of β-blockers varied. Only 1 study reported on adverse events.
Pooled data suggest highly dialyzable β-blockers are associated with similar mortality events and fewer cardiovascular events compared with poorly dialyzable β-blockers.
关于透析患者使用何种β受体阻滞剂存在相互矛盾的证据。本系统评价旨在确定与透析性差的β受体阻滞剂相比,透析性高的β受体阻滞剂是否会使血液透析患者发生心血管事件和死亡的几率更高。
对现有文献进行系统评价。使用所选研究的数据进行荟萃分析。
参与者来自美国、加拿大和台湾。参与者的平均年龄在55.9至75.7岁之间。
我们检索了1990年至2020年9月的Ovid MEDLINE数据库。排除没有成年血液透析参与者以及未对至少两种透析性不同的β受体阻滞剂进行比较的研究。
从每项研究中提取基线和调整后的结局数据。
使用随机效应模型,通过各研究的完全调整模型计算合并风险比。
纳入了四项队列研究。汇总完全调整模型后,与透析性差的β受体阻滞剂相比,透析性高的β受体阻滞剂对死亡率无影响(风险比[HR],0.94;95%置信区间[CI],0.81 - 1.08;I² = 0.84),但与心血管事件减少相关(HR,0.88;95%CI,0.83 - 0.93)。研究之间存在显著异质性(I² = 0.35)。只有一项研究报告了不良事件。与服用美托洛尔(一种透析性高的β受体阻滞剂)的患者相比,服用卡维地洛(一种透析性差的β受体阻滞剂)的患者透析期间低血压更为常见(调整后的发病率比,1.10;95%CI,1.09 - 1.11)。
未找到随机对照试验。每项研究使用了不同的分析方法和结局定义。β受体阻滞剂的分类各不相同。只有一项研究报告了不良事件。
汇总数据表明,与透析性差的β受体阻滞剂相比,透析性高的β受体阻滞剂与死亡率事件相似,但心血管事件较少。