Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, United Kingdom.
Cancer Research UK Oxford Centre, University of Oxford, Oxford, United Kingdom.
JAMA Psychiatry. 2022 Jul 1;79(7):690-698. doi: 10.1001/jamapsychiatry.2022.1067.
Individuals surviving severe COVID-19 may be at increased risk of neuropsychiatric sequelae. Robust assessment of these risks may help improve clinical understanding of the post-COVID syndrome, aid clinical care during the ongoing pandemic, and inform postpandemic planning.
To quantify the risks of new-onset neuropsychiatric conditions and new neuropsychiatric medication prescriptions after discharge from a COVID-19-related hospitalization, and to compare these with risks after discharge from hospitalization for other severe acute respiratory infections (SARI) during the COVID-19 pandemic.
DESIGN, SETTING, AND PARTICIPANTS: In this cohort study, adults (≥18 years of age) were identified from QResearch primary care and linked electronic health record databases, including national SARS-CoV-2 testing, hospital episode statistics, intensive care admissions data, and mortality registers in England, from January 24, 2020, to July 7, 2021.
COVID-19-related or SARI-related hospital admission (including intensive care admission).
New-onset diagnoses of neuropsychiatric conditions (anxiety, dementia, psychosis, depression, bipolar disorder) or first prescription for relevant medications (antidepressants, hypnotics/anxiolytics, antipsychotics) during 12 months of follow-up from hospital discharge. Maximally adjusted hazard ratios (HR) with 95% CIs were estimated using flexible parametric survival models.
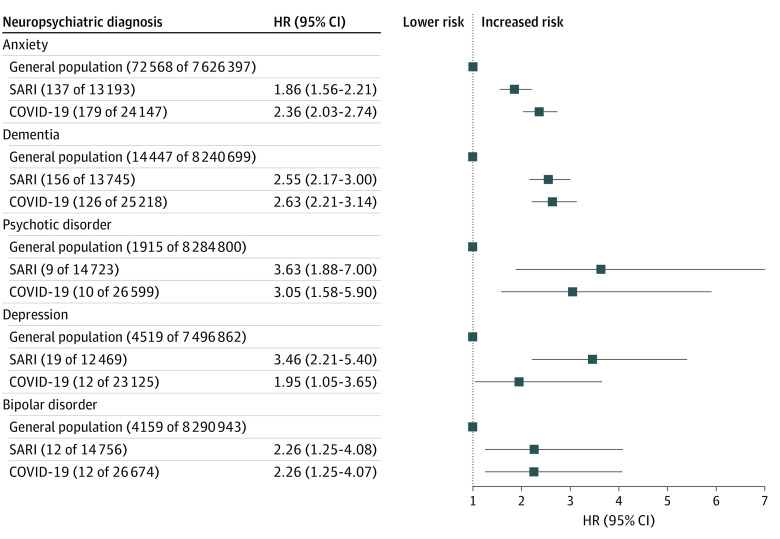
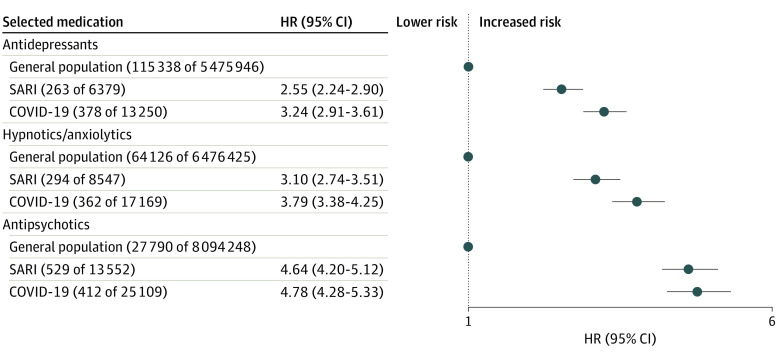
In this cohort study of data from 8.38 million adults (4.18 million women, 4.20 million men; mean [SD] age 49.18 [18.45] years); 16 679 (0.02%) survived a hospital admission for SARI, and 32 525 (0.03%) survived a hospital admission for COVID-19. Compared with the remaining population, survivors of SARI and COVID-19 hospitalization had higher risks of subsequent neuropsychiatric diagnoses. For example, the HR for anxiety in survivors of SARI was 1.86 (95% CI, 1.56-2.21) and for survivors of COVID-19 infection was 2.36 (95% CI, 2.03-2.74); the HR for dementia for survivors of SARI was 2.55 (95% CI, 2.17-3.00) and for survivors of COVID-19 infection was 2.63 (95% CI, 2.21-3.14). Similar findings were observed for all medications analyzed; for example, the HR for first prescriptions of antidepressants in survivors of SARI was 2.55 (95% CI, 2.24-2.90) and for survivors of COVID-19 infection was 3.24 (95% CI, 2.91-3.61). There were no significant differences observed when directly comparing the COVID-19 group with the SARI group apart from a lower risk of antipsychotic prescriptions in the former (HR, 0.80; 95% CI, 0.69-0.92).
In this cohort study, the neuropsychiatric sequelae of severe COVID-19 infection were found to be similar to those for other SARI. This finding may inform postdischarge support for people surviving SARI.
从严重 COVID-19 中幸存下来的个体可能面临神经精神后遗症的风险增加。对这些风险进行全面评估可能有助于提高对 COVID 后综合征的临床认识,在当前大流行期间为临床护理提供帮助,并为大流行后规划提供信息。
量化 COVID-19 相关住院后新发神经精神疾病和新的神经精神药物处方的风险,并与 COVID-19 大流行期间其他严重急性呼吸道感染(SARI)相关住院后出院的风险进行比较。
设计、设置和参与者:在这项队列研究中,从英格兰的 QResearch 初级保健和链接电子健康记录数据库中确定了成年人(≥18 岁),包括全国 SARS-CoV-2 检测、医院发病统计、重症监护入院数据和死亡率登记,时间为 2020 年 1 月 24 日至 2021 年 7 月 7 日。
COVID-19 相关或 SARI 相关的住院(包括重症监护入院)。
在出院后 12 个月的随访期间,新发神经精神疾病(焦虑症、痴呆症、精神病、抑郁症、双相情感障碍)或首次开具相关药物(抗抑郁药、催眠药/抗焦虑药、抗精神病药)的诊断。使用灵活的参数生存模型估计最大调整后的危险比(HR)和 95%置信区间(CI)。
在这项来自 838 万成年人(418 万女性,420 万男性;平均[SD]年龄 49.18[18.45]岁)的队列研究中;16679 人(0.02%)幸存 SARI 住院治疗,32525 人(0.03%)幸存 COVID-19 住院治疗。与剩余人群相比,SARI 和 COVID-19 住院幸存者有更高的后续神经精神诊断风险。例如,SARI 幸存者的焦虑症 HR 为 1.86(95%CI,1.56-2.21),COVID-19 感染幸存者为 2.36(95%CI,2.03-2.74);SARI 幸存者的痴呆症 HR 为 2.55(95%CI,2.17-3.00),COVID-19 感染幸存者为 2.63(95%CI,2.21-3.14)。分析的所有药物都观察到类似的发现;例如,SARI 幸存者首次开抗抑郁药的 HR 为 2.55(95%CI,2.24-2.90),COVID-19 感染幸存者为 3.24(95%CI,2.91-3.61)。除了 COVID-19 组的抗精神病药物处方风险较低(HR,0.80;95%CI,0.69-0.92)外,当直接比较 COVID-19 组和 SARI 组时,没有观察到显著差异。
在这项队列研究中,COVID-19 感染的神经精神后遗症与其他 SARI 相似。这一发现可能为 SARI 幸存者出院后的支持提供信息。