Tranchita Eliana, Murri Arianna, Grazioli Elisa, Cerulli Claudia, Emerenziani Gian Pietro, Ceci Roberta, Caporossi Daniela, Dimauro Ivan, Parisi Attilio
Laboratory of Physical Exercise and Sport Science, Department of Exercise, Human and Health Sciences, University of Rome Foro Italico, Piazza Lauro de Bosis 15, 00135 Rome, Italy.
Department of Experimental and Clinical Medicine, Magna Graecia University, 88100 Catanzaro, Italy.
Cancers (Basel). 2022 May 3;14(9):2288. doi: 10.3390/cancers14092288.
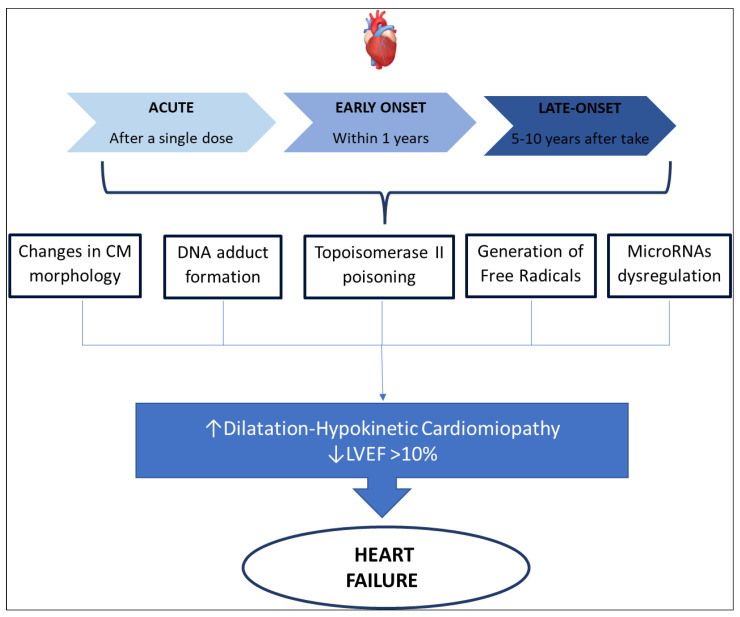
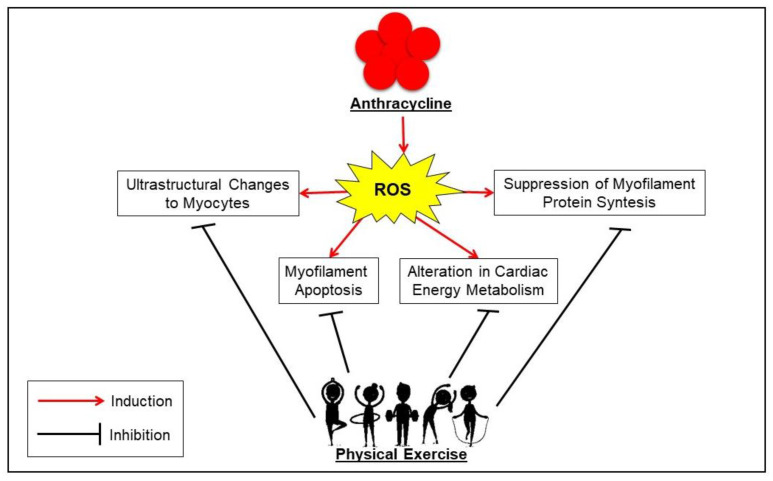
The increase in breast cancer (BC) survival has determined a growing survivor population that seems to develop several comorbidities and, specifically, treatment-induced cardiovascular disease (CVD), especially those patients treated with anthracyclines. Indeed, it is known that these compounds act through the induction of supraphysiological production of reactive oxygen species (ROS), which appear to be central mediators of numerous direct and indirect cardiac adverse consequences. Evidence suggests that physical exercise (PE) practised before, during or after BC treatments could represent a viable non-pharmacological strategy as it increases heart tolerance against many cardiotoxic agents, and therefore improves several functional, subclinical, and clinical parameters. At molecular level, the cardioprotective effects are mainly associated with an exercise-induced increase of stress response proteins (HSP60 and HSP70) and antioxidant (SOD activity, GSH), as well as a decrease in lipid peroxidation, and pro-apoptotic proteins such as Bax, Bax-to-Bcl-2 ratio. Moreover, this protection can potentially be explained by a preservation of myosin heavy chain (MHC) isoform distribution. Despite this knowledge, it is not clear which type of exercise should be suggested in BC patient undergoing anthracycline treatment. This highlights the lack of special guidelines on how affected patients should be managed more efficiently. This review offers a general framework for the role of anthracyclines in the physio-pathological mechanisms of cardiotoxicity and the potential protective role of PE. Finally, potential exercise-based strategies are discussed on the basis of scientific findings.
乳腺癌(BC)生存率的提高导致了幸存者群体的不断增加,这些幸存者似乎出现了多种合并症,特别是治疗引起的心血管疾病(CVD),尤其是那些接受蒽环类药物治疗的患者。事实上,已知这些化合物通过诱导超生理水平的活性氧(ROS)产生而起作用,而ROS似乎是许多直接和间接心脏不良后果的核心介质。有证据表明,在乳腺癌治疗之前、期间或之后进行体育锻炼(PE)可能是一种可行的非药物策略,因为它可以提高心脏对许多心脏毒性药物的耐受性,从而改善一些功能、亚临床和临床参数。在分子水平上,心脏保护作用主要与运动诱导的应激反应蛋白(HSP60和HSP70)和抗氧化剂(超氧化物歧化酶活性、谷胱甘肽)增加有关,同时脂质过氧化以及促凋亡蛋白如Bax、Bax与Bcl-2的比率降低。此外,这种保护作用可能可以通过肌球蛋白重链(MHC)异构体分布的保留来解释。尽管有这些认识,但对于接受蒽环类药物治疗的乳腺癌患者应建议哪种类型的运动尚不清楚。这突出表明缺乏关于如何更有效地管理受影响患者的特殊指南。本综述为蒽环类药物在心脏毒性生理病理机制中的作用以及体育锻炼的潜在保护作用提供了一个总体框架。最后,根据科学发现讨论了基于运动的潜在策略。