Hawranko Robert, Sohn James J, Neiderer Keith, Bump Ed, Harris Timothy, Fields Emma C, Weiss Elisabeth, Song William Y
Department of Radiation Oncology, Virginia Commonwealth University, Richmond, VA 23226, USA.
Department of Radiation Oncology, Northwestern University Feinberg School of Medicine, Chicago, IL 60611, USA.
J Clin Med. 2022 May 5;11(9):2584. doi: 10.3390/jcm11092584.
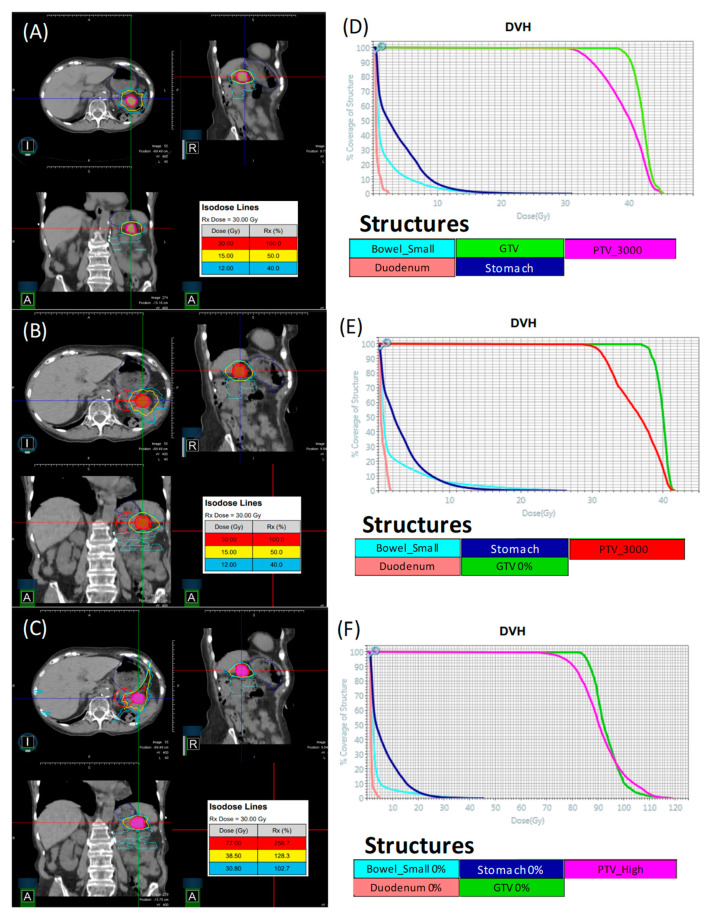
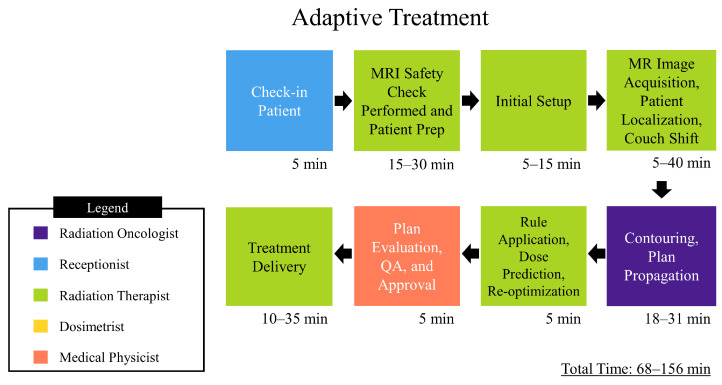
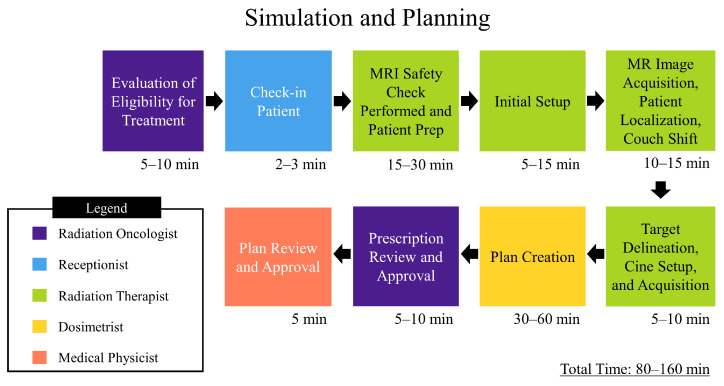
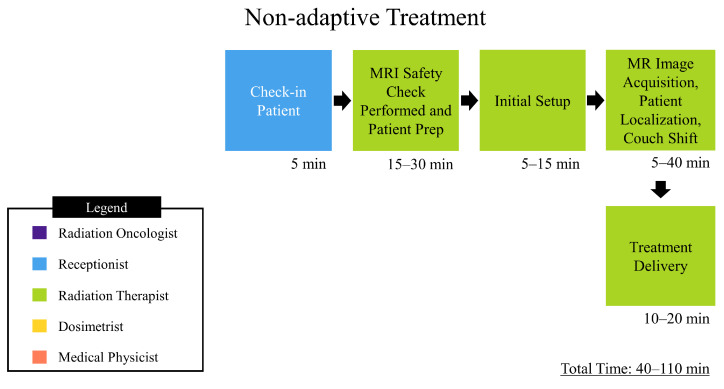
This study investigates plan quality generated by an MR-Linac (MRL) treatment planning system (TPS) for 5-fraction stereotactic body radiation therapy (SBRT) of primary pancreatic cancer (PCa). In addition, an isotoxic dose escalation was investigated with the MRL TPS based on stereotactic MR-guided adaptive radiation therapy (SMART) trial constraints. A clinical workflow was developed for adaptive and non-adaptive treatments with the MRL, on which a time-driven activity-based costing (TDABC) analysis was performed to quantify clinical efficacy. Fifteen PCa patients previously treated with a conventional Linac were retrospectively re-planned for this study. Three plans were generated for each patient using the original prescription dose (PD) and organ at risk (OAR) constraints (Plan 1), following SMART trial's OAR constraints but with the original PD (Plan 2), starting with Plan 2, following an isotoxic dose escalation strategy where the dose was escalated until any one of the SMART trial's OAR constraints reached its limit (Plan 3). Conformity index (CI) and the ratio of the 50% isodose volume to PTV (R50%) conformity metrics were calculated for all 45 MRL plans, in addition to standard dose-volume indices. Forty-five MRL plans were created which met their respective dosimetric criteria described above. For Plan 1, the MRL TPS successfully achieved equivalent or lower OAR doses while maintaining the prescribed PTV coverage for the 15 plans. A maximum dose to the small bowel was reduced on average by 4.97 Gy (range: 1.11-10.58 Gy). For Plan 2, the MRL TPS successfully met all SMART trial OAR constraints while maintaining equivalent PTV coverage. For Plan 3, the MRL TPS was able to escalate the prescription dose from the original 25-33 Gy by, on average, 36 Gy (range: 15-70 Gy), and dose to the PTV was successfully escalated to at least 50 Gy for all 15 plans. These achievements were made possible, in part, due to the omission of the ITV afforded by the MRL's real-time target tracking technology and sharper dose penumbra due to its unique dual-focus MLC design. The 0.35T MRL TPS can generate plans that are equivalent to conventional Linac-based plans for SBRT of PCa. Through analyzing Plan 2 and 3 strategies, and due to the real-time target localization capabilities of the MRL system, increased OAR sparing and/or target dose escalation are possible.
本研究调查了磁共振直线加速器(MR-Linac)治疗计划系统(TPS)针对原发性胰腺癌(PCa)的5分次立体定向体部放射治疗(SBRT)所生成的计划质量。此外,基于立体定向磁共振引导自适应放射治疗(SMART)试验的限制条件,使用MR-Linac TPS研究了等毒性剂量递增。开发了一种用于MR-Linac自适应和非自适应治疗的临床工作流程,并在此基础上进行了基于时间驱动的作业成本法(TDABC)分析以量化临床疗效。对15例先前接受传统直线加速器治疗的PCa患者进行回顾性重新计划用于本研究。每位患者使用原始处方剂量(PD)和危及器官(OAR)限制条件生成三个计划(计划1),遵循SMART试验的OAR限制条件但使用原始PD(计划2),从计划2开始,遵循等毒性剂量递增策略,即剂量递增直至SMART试验的任何一个OAR限制条件达到其极限(计划3)。除了标准剂量体积指数外,还计算了所有45个MR-Linac计划的适形指数(CI)以及50%等剂量体积与计划靶体积(PTV)的比值(R50%)适形指标。创建了45个符合上述各自剂量学标准的MR-Linac计划。对于计划1,MR-Linac TPS成功实现了等效或更低的OAR剂量,同时维持了15个计划中规定的PTV覆盖范围。小肠的最大剂量平均降低了4.97 Gy(范围:1.11 - 10.58 Gy)。对于计划2,MR-Linac TPS成功满足了所有SMART试验的OAR限制条件,同时维持了等效的PTV覆盖范围。对于计划3,MR-Linac TPS能够将处方剂量从原始的25 - 33 Gy平均递增36 Gy(范围:15 - 70 Gy),并且对于所有15个计划,PTV的剂量成功递增至至少50 Gy。这些成果部分得益于MR-Linac实时靶区跟踪技术所带来的内部靶区体积(ITV)的省略以及其独特的双焦点多叶准直器(MLC)设计所产生的更清晰的剂量半影。0.35T的MR-Linac TPS能够生成与基于传统直线加速器的PCa SBRT计划等效的计划。通过分析计划2和3的策略,并且由于MR-Linac系统的实时靶区定位能力,增加OAR保护和/或靶区剂量递增是可行的。