Nuñez-Garcia Jean C, Sánchez-Puente Antonio, Sampedro-Gómez Jesús, Vicente-Palacios Victor, Jiménez-Navarro Manuel, Oterino-Manzanas Armando, Jiménez-Candil Javier, Dorado-Diaz P Ignacio, Sánchez Pedro L
Department of Cardiology, Hospital Universitario de Salamanca-IBSAL, 37007 Salamanca, Spain.
CIBERCV (Centro de Investigacion Biomedica en Red Enfermedades Cardiovasculares), Instituto de Salud Carlos III, C/Monforte de Lemos 3-5, Pabellón 11, Planta 0, 28029 Madrid, Spain.
J Clin Med. 2022 May 7;11(9):2636. doi: 10.3390/jcm11092636.
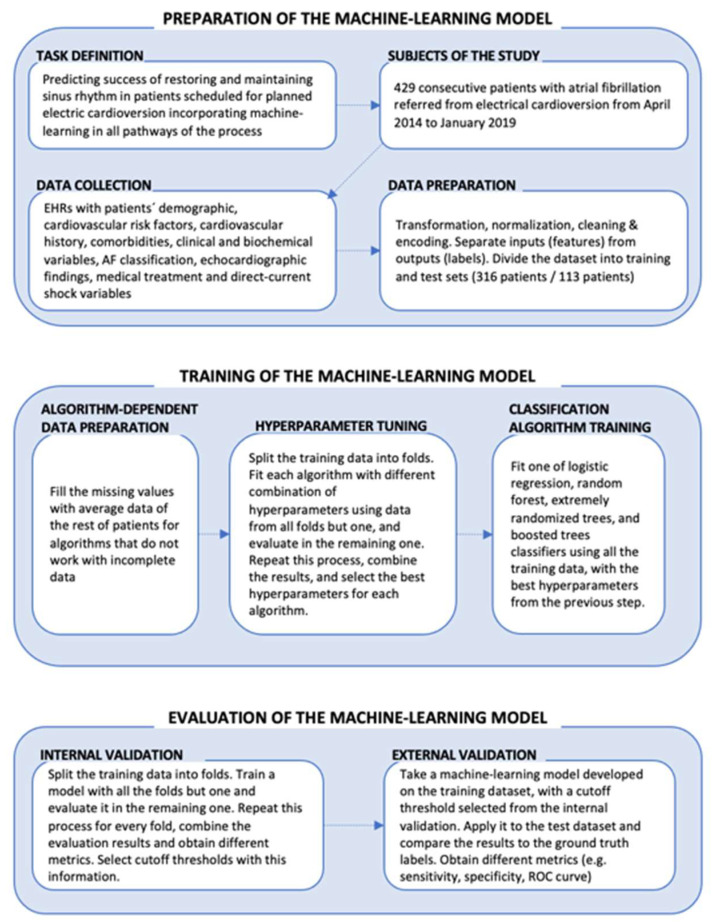
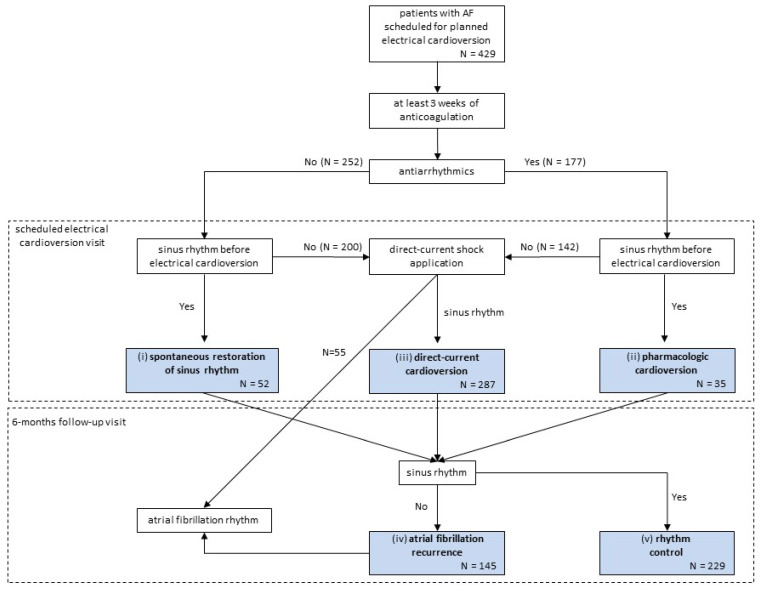
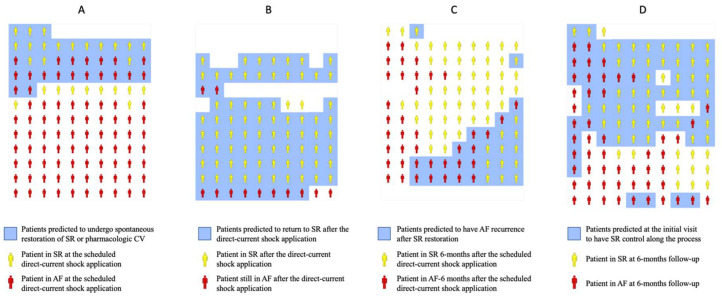
Background: The integrated approach to electrical cardioversion (EC) in atrial fibrillation (AF) is complex; candidates can resolve spontaneously while waiting for EC, and post-cardioversion recurrence is high. Thus, it is especially interesting to avoid the programming of EC in patients who would restore sinus rhythm (SR) spontaneously or present early recurrence. We have analyzed the whole elective EC of the AF process using machine-learning (ML) in order to enable a more realistic and detailed simulation of the patient flow for decision making purposes. Methods: The dataset consisted of electronic health records (EHRs) from 429 consecutive AF patients referred for EC. For analysis of the patient outcome, we considered five pathways according to restoring and maintaining SR: (i) spontaneous SR restoration, (ii) pharmacologic-cardioversion, (iii) direct-current cardioversion, (iv) 6-month AF recurrence, and (v) 6-month rhythm control. We applied ML classifiers for predicting outcomes at each pathway and compared them with the CHA2DS2-VASc and HATCH scores. Results: With the exception of pathway (iii), all ML models achieved improvements in comparison with CHA2DS2-VASc or HATCH scores (p < 0.01). Compared to the most competitive score, the area under the ROC curve (AUC-ROC) was: 0.80 vs. 0.66 for predicting (i); 0.71 vs. 0.55 for (ii); 0.64 vs. 0.52 for (iv); and 0.66 vs. 0.51 for (v). For a threshold considered optimal, the empirical net reclassification index was: +7.8%, +47.2%, +28.2%, and +34.3% in favor of our ML models for predicting outcomes for pathways (i), (ii), (iv), and (v), respectively. As an example tool of generalizability of ML models, we deployed our algorithms in an open-source calculator, where the model would personalize predictions. Conclusions: An ML model improves the accuracy of restoring and maintaining SR predictions over current discriminators. The proposed approach enables a detailed simulation of the patient flow through personalized predictions.
心房颤动(AF)的电复律(EC)综合方法较为复杂;候选患者在等待电复律期间可能会自行恢复,且复律后复发率较高。因此,对于那些能自行恢复窦性心律(SR)或早期复发的患者,避免安排电复律尤其有意义。我们使用机器学习(ML)分析了整个AF过程的择期电复律,以便为决策目的更真实、详细地模拟患者流程。方法:数据集包括429例连续接受电复律的AF患者的电子健康记录(EHRs)。为分析患者结局,我们根据恢复和维持SR考虑了五种途径:(i)自发恢复SR,(ii)药物复律,(iii)直流电复律,(iv)6个月AF复发,以及(v)6个月心律控制。我们应用ML分类器预测各途径的结局,并将其与CHA2DS2-VASc和HATCH评分进行比较。结果:除途径(iii)外,所有ML模型与CHA2DS2-VASc或HATCH评分相比均有改善(p < 0.01)。与最具竞争力的评分相比,预测(i)时ROC曲线下面积(AUC-ROC)为:0.80对0.66;预测(ii)时为0.71对0.55;预测(iv)时为0.64对0.52;预测(v)时为0.66对0.51。对于认为最佳的阈值,经验性净重新分类指数分别为:支持我们的ML模型预测途径(i)、(ii)、(iv)和(v)结局的+7.8%、+47.2%、+28.2%和+34.3%。作为ML模型可推广性的一个示例工具,我们将算法部署在一个开源计算器中,该模型将进行个性化预测。结论:ML模型比当前的判别方法提高了恢复和维持SR预测的准确性。所提出的方法通过个性化预测实现了对患者流程的详细模拟。