The Permanente Medical Group, Oakland, California.
Kaiser Permanente Division of Research, Oakland, California.
JAMA Netw Open. 2022 May 2;5(5):e2212340. doi: 10.1001/jamanetworkopen.2022.12340.
Physicians commonly hospitalize patients presenting to the emergency department (ED) with acute pulmonary embolism (PE), despite eligibility for safe outpatient management. Risk stratification using electronic health record-embedded clinical decision support systems can aid physician site-of-care decision-making and increase safe outpatient management. The long-term sustainability of early improvements after the cessation of trial-based, champion-led promotion is uncertain.
To evaluate the sustainability of recommended site-of-care decision-making support 4 years after initial physician champion-led interventions to increase outpatient management for patients with acute PE.
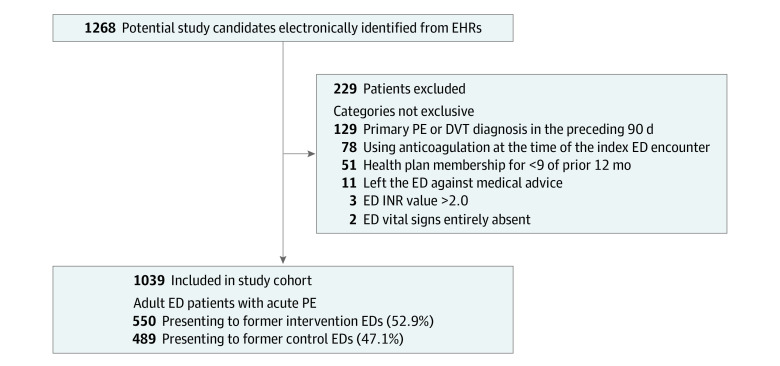
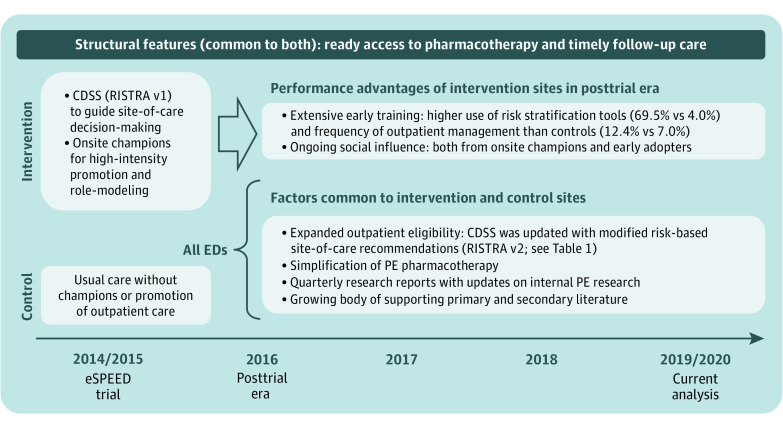
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study was conducted in 21 US community hospitals in an integrated health system. Participants included adult patients presenting to the ED with acute PE. Study sites had participated in an original decision-support intervention trial 4 years prior to the current study period: 10 sites were intervention sites, 11 sites were controls. In that trial, decision support with champion promotion resulted in significantly higher outpatient management at intervention sites compared with controls. After trial completion, all study sites were given continued access to a modified decision-support tool without further champion-led outreach. Data were analyzed from January 2019 to February 2020.
ED treatment with a modified clinical decision support tool.
The main outcome was frequency of outpatient management, defined as discharge home directly from the ED, stratified by the PE Severity Index. The safety measure of outpatient care was 7-day PE-related hospitalization.
This study included 1039 patients, including 533 (51.3%) women, with a median (IQR) age of 65 (52-74) years. Nearly half (474 patients [45.6%]) were rated lower risk on the PE Severity Index. Overall, 278 patients (26.8%) were treated as outpatients, with only four 7-day PE-related hospitalizations (1.4%; 95% CI, 0.4%-3.6%). The practice gap in outpatient management created by the earlier trial persisted in the outpatient management for patients with lower risk: 109 of 236 patients (46.2%) at former intervention sites vs 81 of 238 patients (34.0%) at former control sites (difference, 12.2; [95% CI, 3.4-20.9] percentage points; P = .007), with wide interfacility variation (range, 7.1%-47.1%).
In this cohort study, a champion-led, decision-support intervention to increase outpatient management for patients presenting to the ED with acute pulmonary embolism was associated with sustained higher rates of outpatient management 4 years later. The application of our findings to improving sustainability of practice change for other clinical conditions warrants further study.
尽管适合安全的门诊管理,但医生通常会将急性肺栓塞(PE)患者收入急诊病房(ED)。使用电子病历嵌入式临床决策支持系统进行风险分层有助于医生做出治疗地点决策,并增加安全的门诊管理。在基于试验的、冠军领导的推广停止后,早期改进的长期可持续性是不确定的。
评估在最初由医生冠军领导的干预措施增加急性 PE 患者门诊管理 4 年后,推荐的治疗地点决策支持的可持续性。
设计、地点和参与者:这是一项回顾性队列研究,在一个综合医疗系统的 21 家美国社区医院进行。参与者包括在 ED 就诊的急性 PE 成年患者。研究地点在前一个研究期间参加了一项原始决策支持干预试验 4 年:10 个地点为干预地点,11 个地点为对照地点。在该试验中,与对照组相比,决策支持与冠军推广显著提高了干预地点的门诊管理。试验完成后,所有研究地点都可以继续使用修改后的决策支持工具,而无需进一步的冠军领导外联。数据于 2019 年 1 月至 2020 年 2 月进行分析。
ED 采用改良的临床决策支持工具治疗。
主要结局是门诊管理的频率,定义为直接从 ED 出院回家,按 PE 严重指数分层。门诊护理的安全性措施是 7 天内与 PE 相关的住院治疗。
这项研究包括 1039 名患者,其中 533 名(51.3%)为女性,中位(IQR)年龄为 65(52-74)岁。近一半(474 名患者[45.6%])在 PE 严重指数上的风险评分较低。总体而言,278 名患者(26.8%)接受了门诊治疗,只有 4 名患者在 7 天内因 PE 相关住院(1.4%;95%CI,0.4%-3.6%)。早期试验造成的门诊管理实践差距在低风险患者的门诊管理中仍然存在:前干预地点的 236 名患者中有 109 名(46.2%),前对照地点的 238 名患者中有 81 名(34.0%)(差异,12.2;[95%CI,3.4-20.9]个百分点;P=0.007),各医疗机构之间存在很大差异(范围为 7.1%-47.1%)。
在这项队列研究中,一项由冠军领导的、以决策支持为基础的干预措施,旨在增加因急性肺栓塞就诊的 ED 患者的门诊管理,4 年后与更高的门诊管理率持续相关。将我们的研究结果应用于改善其他临床条件下实践变革的可持续性,值得进一步研究。