Department of Pediatrics, Mikkeli Central Hospital, Mikkeli, Finland.
Institute of Clinical Medicine and Department of Pediatrics, University of Eastern Finland, Kuopio, Finland.
Clin Infect Dis. 2023 Feb 8;76(3):e1123-e1128. doi: 10.1093/cid/ciac374.
The optimal treatment duration of community-acquired pneumonia (CAP) in children has been controversial in high-income countries. We conducted a meta-analysis to compare short antibiotic treatment (3-5 days) with longer treatment (7-10 days) among children aged ≥6 months.
On 31 January 2022, we searched PubMed, Scopus, and Web of Science databases for studies published in English from 2003 to 2022. We included randomized controlled trials focusing on antibiotic treatment duration in children with CAP treated as outpatients. We calculated risk differences (RDs) with 95% confidence intervals and used the fixed-effect model (low heterogeneity). Our main outcome was treatment failure, defined as need for retreatment or hospitalization within 1 month. Our secondary outcome was presence of antibiotic-related harms.
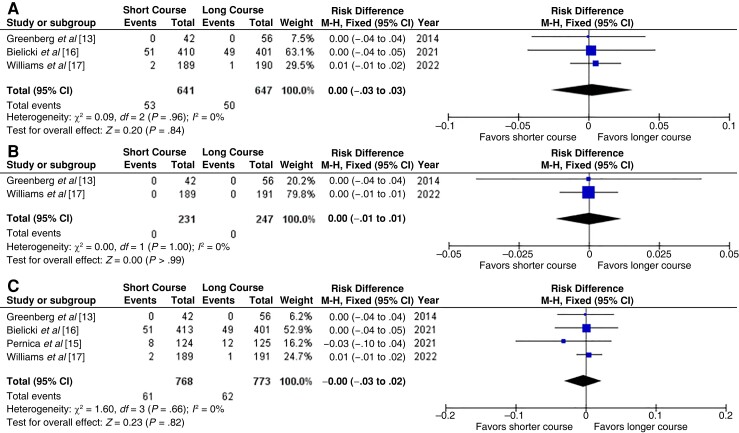
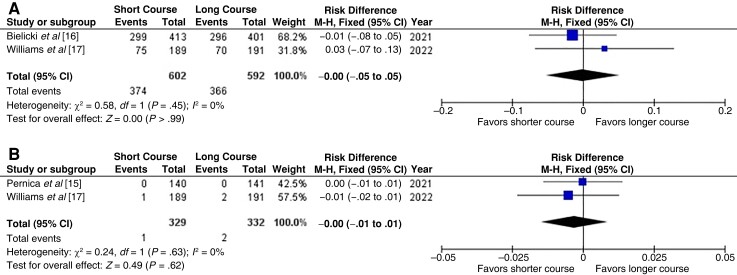
A total of 541 studies were screened, and 4 studies with 1541 children were included in the review. Three studies had low risk of bias, and one had some concerns. All 4 studies assessed treatment failures, and the RD was 0.1% (95% confidence interval, -3.0% to 2.0%) with high quality of evidence. Two studies (1194 children) assessed adverse events related to antibiotic treatment, and the RD was 0.0% (-5.0% to 5.0%) with moderate quality of evidence. The diagnostic criteria varied between the included studies.
A short antibiotic treatment duration of 3-5 days was equally effective and safe compared with the longer (current) recommendation of 7-10 days in children aged ≥6 months with CAP. We suggest that short antibiotic courses can be implemented in treatment of pediatric CAP.
在高收入国家,儿童获得性肺炎(CAP)的最佳治疗持续时间一直存在争议。我们进行了一项荟萃分析,比较了≥6 个月儿童中短期(3-5 天)和长期(7-10 天)抗生素治疗的效果。
2022 年 1 月 31 日,我们检索了 PubMed、Scopus 和 Web of Science 数据库中 2003 年至 2022 年发表的英文文献。我们纳入了以门诊治疗 CAP 的儿童抗生素治疗持续时间为重点的随机对照试验。我们计算了风险差异(RD)及其 95%置信区间,并使用固定效应模型(低异质性)。我们的主要结局是治疗失败,定义为 1 个月内需要再次治疗或住院。次要结局为抗生素相关危害的发生情况。
共筛选出 541 篇研究,其中 4 项研究(1541 名儿童)纳入综述。3 项研究的偏倚风险较低,1 项研究存在一些关注。4 项研究均评估了治疗失败情况,高质量证据显示 RD 为 0.1%(95%置信区间,-3.0%至 2.0%)。2 项研究(1194 名儿童)评估了与抗生素治疗相关的不良事件,中质量证据显示 RD 为 0.0%(-5.0%至 5.0%)。纳入研究的诊断标准存在差异。
与目前推荐的 7-10 天相比,≥6 个月儿童 CAP 的 3-5 天短疗程抗生素治疗同样有效且安全。我们建议在治疗儿科 CAP 时可以采用短疗程抗生素治疗。