Centre for Academic Child Health, Bristol Medical School, University of Bristol, Canynge Hall, 39 Whatley Road, Bristol, BS8 2PS, UK.
Department of Population Health Sciences, Bristol Medical School, University of Bristol, Bristol, UK.
Eur J Nutr. 2022 Oct;61(7):3471-3486. doi: 10.1007/s00394-022-02860-9. Epub 2022 May 20.
This study examined the association between a Dietary Inflammatory Score adapted for children (cDIS) and Cardiometabolic Risk (CMR) score in adolescence/early adulthood in the Avon Longitudinal Study of Parents and Children (ALSPAC).
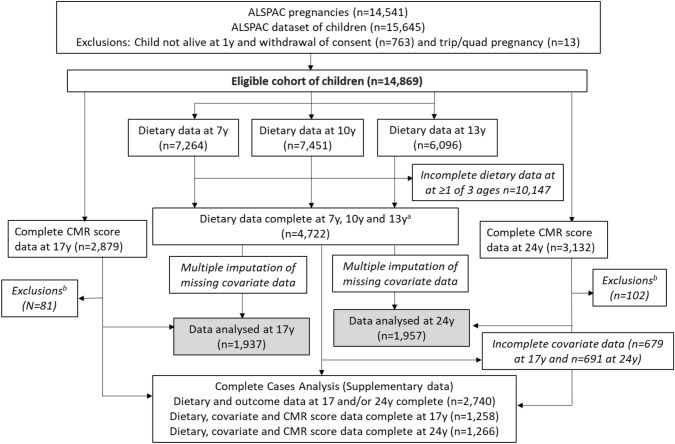
The cDIS was calculated at 7, 10 and 13 years using diet diary data. Anthropometric and biochemical data at 17 (N = 1937) and 24 (N = 1957) years were used to calculate CMR scores at each age [mean sex-specific z-scores from triacylglycerol, HDL-cholesterol, LDL-cholesterol, mean arterial blood pressure (MAP), homeostatic model assessment of insulin resistance (HOMA-IR) and fat-mass index (FMI)]. Multivariable linear regression models examined associations between cDIS at 7, 10 and 13 years and a continuous CMR z-score and individual CMR markers at 17 and 24 years.
In fully adjusted models, a higher cDIS (more pro-inflammatory diet) at 7 years was associated with an increase in CMR z-score at 17 years (β 0.19; 95% CI 0.03-0.35 for third versus first cDIS tertile) and at 24 years (β 0.28; 95% CI 0.11,0.44 for third versus first cDIS tertile). There was a weak association between a higher cDIS at 10 years and an increase in CMR z-score at 17 years (β 0.16; 95% CI - 0.003, 0.32 for third versus first cDIS tertile). No other clear associations were evident. FMI, MAP and HOMA-IR were the main CMR factors contributing to these associations.
A more pro-inflammatory diet during childhood was associated with a worse cardiometabolic profile in late adolescence/early adulthood. A childhood diet abundant in nutrients with anti-inflammatory properties could help reduce development of CMR factors.
本研究旨在探讨儿童饮食炎症评分(cDIS)与青少年/成年早期心血管代谢风险(CMR)评分之间的关系,该研究基于阿冯纵向父母与子女研究(ALSPAC)。
通过饮食日记数据,在 7、10 和 13 岁时计算 cDIS。在 17 岁(N=1937)和 24 岁(N=1957)时,使用人体测量和生化数据来计算每个年龄的 CMR 评分[三酰甘油、高密度脂蛋白胆固醇、低密度脂蛋白胆固醇、平均动脉血压(MAP)、稳态模型评估的胰岛素抵抗(HOMA-IR)和脂肪质量指数(FMI)的性别特异性均数 z 分数]。多变量线性回归模型分析了 7、10 和 13 岁时的 cDIS 与 17 和 24 岁时的连续 CMR z 评分和个别 CMR 标志物之间的关系。
在完全调整的模型中,7 岁时较高的 cDIS(促炎饮食较多)与 17 岁时 CMR z 评分的增加相关(β 0.19;第三与第一 cDIS 三分位组相比,95%CI 为 0.03-0.35)和 24 岁时(β 0.28;95%CI 为 0.11,0.44,第三与第一 cDIS 三分位组相比)。10 岁时较高的 cDIS 与 17 岁时 CMR z 评分的增加之间存在较弱的关联(β 0.16;95%CI 为-0.003,0.32,第三与第一 cDIS 三分位组相比)。没有其他明显的关联。FMI、MAP 和 HOMA-IR 是这些关联的主要 CMR 因素。
儿童期更促炎的饮食与青少年晚期/成年早期的心血管代谢状况较差有关。富含具有抗炎特性的营养物质的儿童饮食可能有助于减少 CMR 因素的发展。