Yang Zhiqi, Lin Daiying, Chen Xiaofeng, Qiu Jinming, Li Shengkai, Huang Ruibin, Yang Zhijian, Sun Hongfu, Liao Yuting, Xiao Jianning, Tang Yanyan, Chen Xiangguang, Zhang Sheng, Dai Zhuozhi
Department of Radiology, Meizhou People's Hospital, Meizhou, China.
Department of Radiology, Shantou Central Hospital, Shantou, China.
Front Microbiol. 2022 May 6;13:847836. doi: 10.3389/fmicb.2022.847836. eCollection 2022.
Both coronavirus disease 2019 (COVID-19) and influenza pneumonia are highly contagious and present with similar symptoms. We aimed to identify differences in CT imaging and clinical features between COVID-19 and influenza pneumonia in the early stage and to identify the most valuable features in the differential diagnosis.
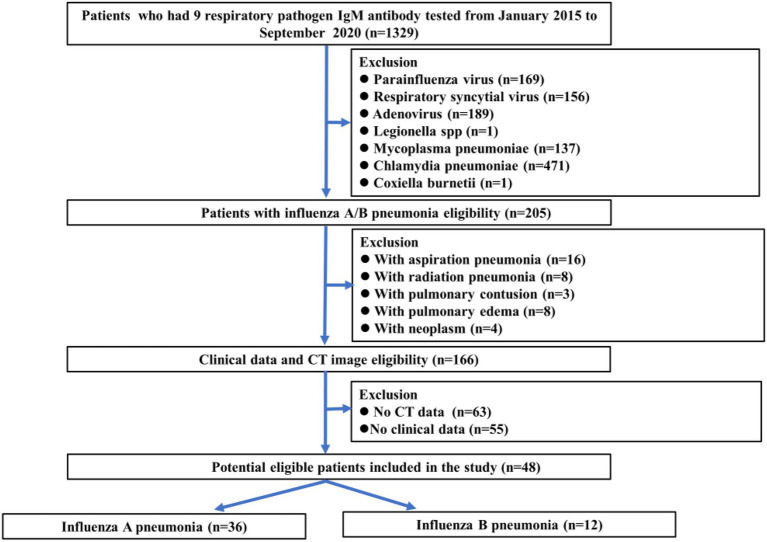
Seventy-three patients with COVID-19 confirmed by real-time reverse transcription-polymerase chain reaction (RT-PCR) and 48 patients with influenza pneumonia confirmed by direct/indirect immunofluorescence antibody staining or RT-PCR were retrospectively reviewed. Clinical data including course of disease, age, sex, body temperature, clinical symptoms, total white blood cell (WBC) count, lymphocyte count, lymphocyte ratio, neutrophil count, neutrophil ratio, and C-reactive protein, as well as 22 qualitative and 25 numerical imaging features from non-contrast-enhanced chest CT images were obtained and compared between the COVID-19 and influenza pneumonia groups. Correlation tests between feature metrics and diagnosis outcomes were assessed. The diagnostic performance of each feature in differentiating COVID-19 from influenza pneumonia was also evaluated.
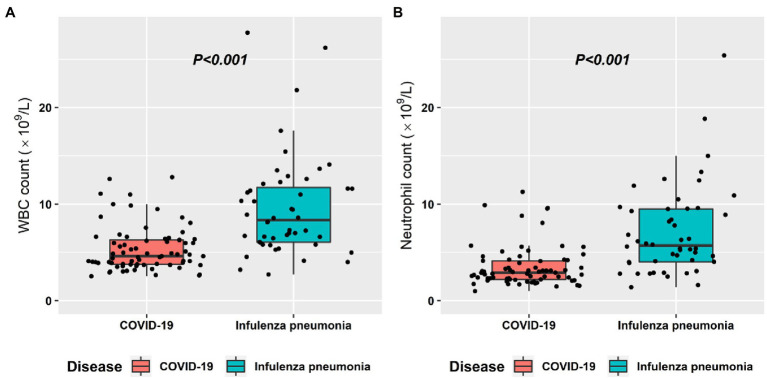
Seventy-three COVID-19 patients including 41 male and 32 female with mean age of 41.9 ± 14.1 and 48 influenza pneumonia patients including 30 male and 18 female with mean age of 40.4 ± 27.3 were reviewed. Temperature, WBC count, crazy paving pattern, pure GGO in peripheral area, pure GGO, lesion sizes (1-3 cm), emphysema, and pleural traction were significantly independent associated with COVID-19. The AUC of clinical-based model on the combination of temperature and WBC count is 0.880 (95% CI: 0.819-0.940). The AUC of radiological-based model on the combination of crazy paving pattern, pure GGO in peripheral area, pure GGO, lesion sizes (1-3 cm), emphysema, and pleural traction is 0.957 (95% CI: 0.924-0.989). The AUC of combined model based on the combination of clinical and radiological is 0.991 (95% CI: 0.980-0.999).
COVID-19 can be distinguished from influenza pneumonia based on CT imaging and clinical features, with the highest AUC of 0.991, of which crazy-paving pattern and WBC count play most important role in the differential diagnosis.
2019冠状病毒病(COVID-19)和流感肺炎均具有高度传染性,且症状相似。我们旨在确定COVID-19和流感肺炎早期CT影像学及临床特征的差异,并找出鉴别诊断中最有价值的特征。
回顾性分析73例经实时逆转录-聚合酶链反应(RT-PCR)确诊的COVID-19患者和48例经直接/间接免疫荧光抗体染色或RT-PCR确诊的流感肺炎患者。获取包括病程、年龄、性别、体温、临床症状、白细胞(WBC)总数、淋巴细胞计数、淋巴细胞比例、中性粒细胞计数、中性粒细胞比例及C反应蛋白等临床数据,以及非增强胸部CT图像的22项定性和25项定量影像学特征,并在COVID-19组和流感肺炎组之间进行比较。评估特征指标与诊断结果之间的相关性检验。还评估了每项特征在鉴别COVID-19与流感肺炎中的诊断性能。
共回顾了73例COVID-19患者(男性41例,女性32例,平均年龄41.9±14.1岁)和48例流感肺炎患者(男性30例,女性18例,平均年龄40.4±27.3岁)。体温、WBC计数、铺路石样改变、外周区域单纯磨玻璃影、单纯磨玻璃影、病灶大小(1-3cm)、肺气肿及胸膜牵拉与COVID-19显著独立相关。基于体温和WBC计数联合的临床模型的AUC为0.880(95%CI:0.819-0.940)。基于铺路石样改变、外周区域单纯磨玻璃影、单纯磨玻璃影、病灶大小(1-3cm)、肺气肿及胸膜牵拉联合的影像学模型的AUC为0.957(95%CI:0.924-0.989)。基于临床和影像学联合的联合模型的AUC为0.991(95%CI:0.980-0.999)。
基于CT影像学和临床特征可将COVID-19与流感肺炎区分开来,最高AUC为0.991,其中铺路石样改变和WBC计数在鉴别诊断中起最重要作用。