Department of Nephrology, Third Xiangya Hospital, Central South University, Changsha, China.
Department of Nephrology, Yueyang People's Hospital, Yueyang Hospital affiliated to Hunan Normal University, Yueyang, China.
Ren Fail. 2022 Dec;44(1):862-880. doi: 10.1080/0886022X.2022.2079522.
The role of probiotics in the management of diabetic kidney disease (DKD) has been shown. Several current trials are investigating the effect of probiotics, which are widely used to modulate biomarkers of renal function, glucose, lipids, inflammation and oxidative stress in patients with DKD. However, their findings are controversial. This study aimed to systematically evaluate the impact of probiotics on patients with DKD meta-analysis.
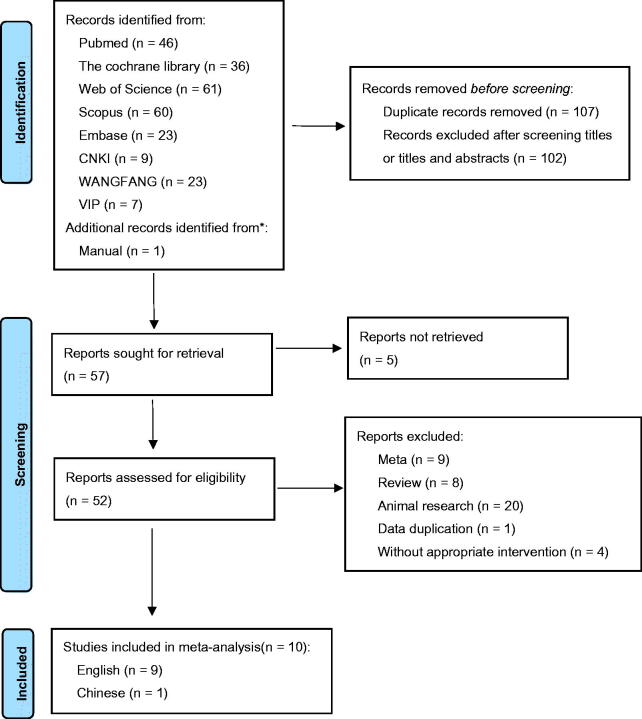
PubMed, The Cochrane Library, Web of Science, Scopus, Embase, China National Knowledge Infrastructure, Chinese Wanfang Database and Chinese VIP Database were searched for relevant studies from the establishment of these databases to September 2021. The pooled results evaluated the impact of probiotics on renal function, glucose, lipids, inflammation and oxidative stress indicators in patients with DKD. Additionally, subgroup analysis was performed based on intervention duration, probiotic dose and probiotic consumption patterns, respectively.
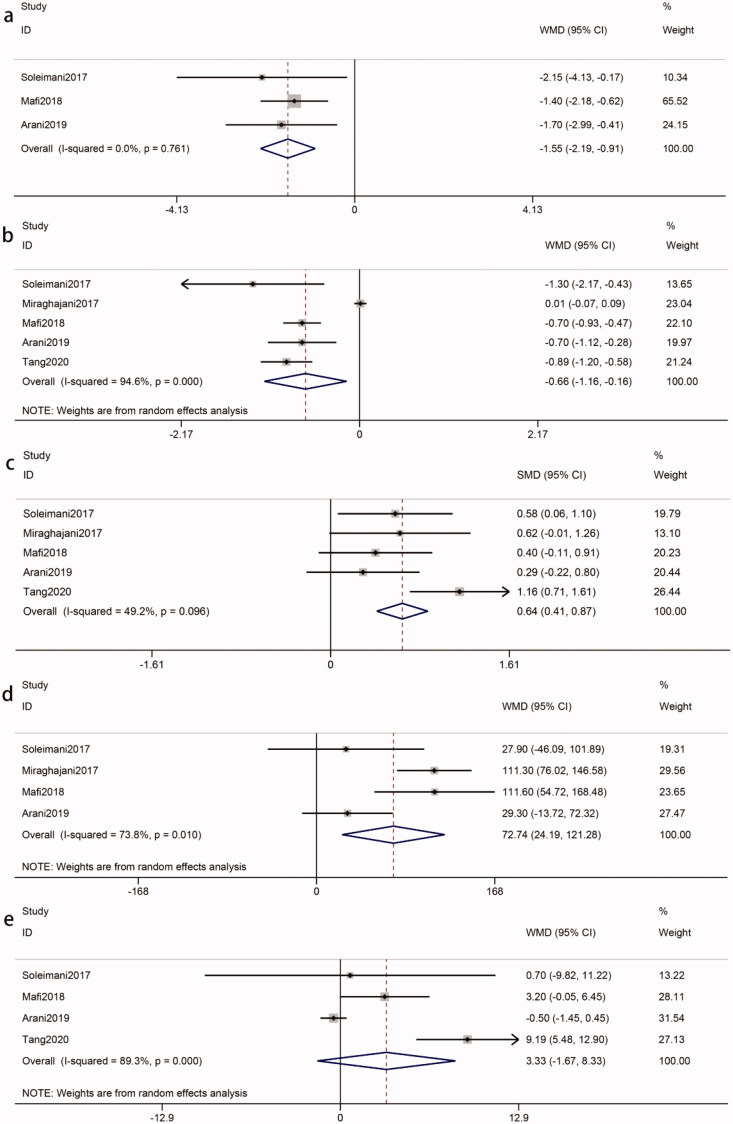
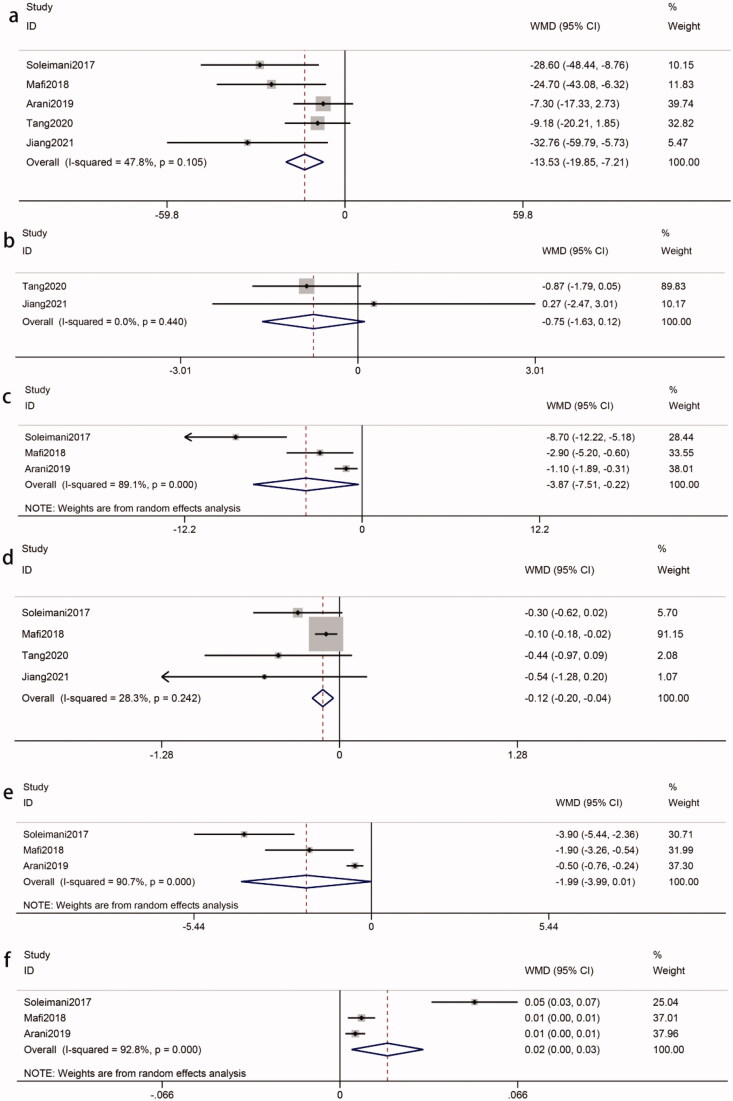
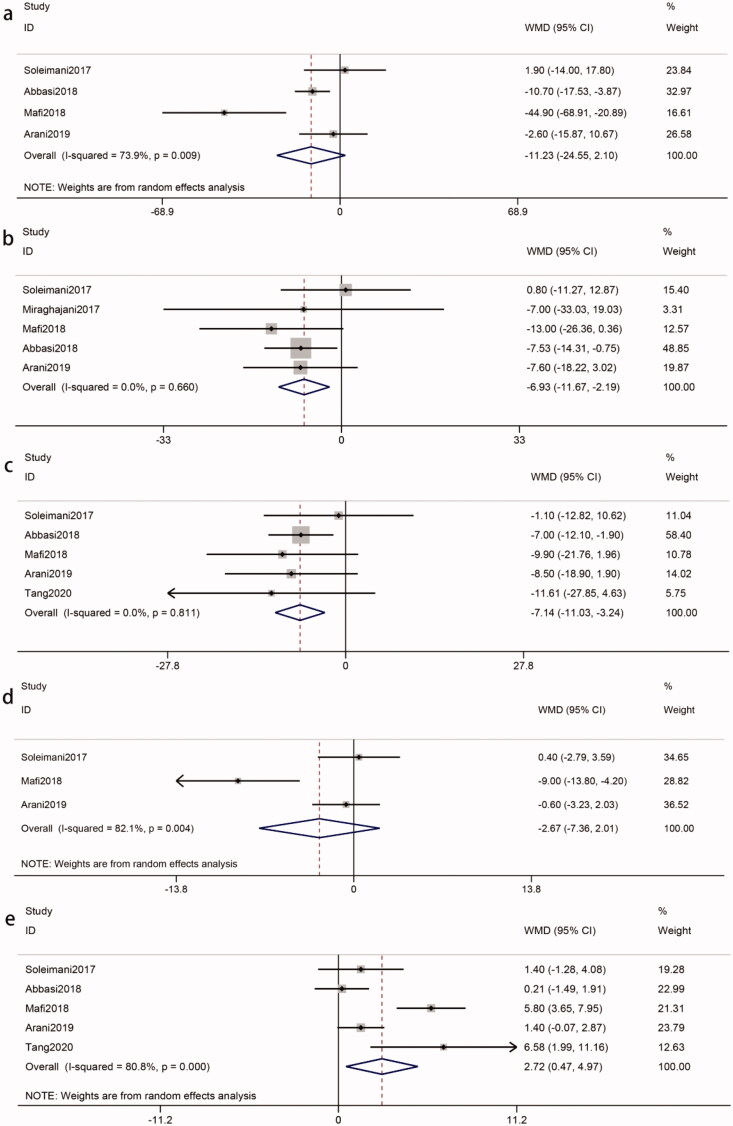
Ten trials that included 552 participants were identified for analysis. Compared with the controls, probiotics significantly decreased serum creatinine (Scr) [WMD = -0.17 mg/dL; 95%CI = -0.29, -0.05; = 0.004], blood urea nitrogen (BUN) [WMD = -1.36 mg/dL; 95%CI = -2.20, -0.52; = 0.001], cystatin C (Cys C) [WMD = -29.50 ng/mL; 95%CI = -32.82, -26.18; < 0.00001], urinary albumin/creatinine ratio (UACR) [WMD = -16.05 mg/g; 95%CI = -27.12, -4.99; = 0.004] and natrium (Na) [WMD = -0.94 mmol/L; 95%CI = -1.82, -0.05; = 0.04] in patients with DKD. Enhanced glycemic control was observed in patients with DKD receiving probiotics compared with controls, as demonstrated by reduced levels of fasting plasma glucose (FPG), hemoglobin A1c (HbA1c), homeostasis model of assessment-estimated insulin resistance (HOMA-IR), and increased quantitative insulin sensitivity check index (QUICKI). Probiotics affected lipid metabolism parameters with decreasing triglycerides (TG), total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-c) levels in patients with DKD. Probiotics could also could improve inflammation and oxidative stress by decreasing high-sensitivity C-reactive protein (hs-CRP), plasma malondialdehyde (MDA), total antioxidant capacity (TAC), glutathione (GSH) and nitric oxide (NO). Additionally, subgroup analysis showed that those who received multiple species probiotics had a statistically significant difference in BUN, FPG, HOMA-IR, high-density lipoprotein cholesterol (HDL-c), MDA, TAC, and NO. Meanwhile, Scr, LDL-c, HDL-c, MDA, and TAC were ameliorated when the intervention duration was more than eight weeks and BUN, FPG, HOMA-IR, and MDA were improved when the probiotic dose was greater than four billion CFU/day.
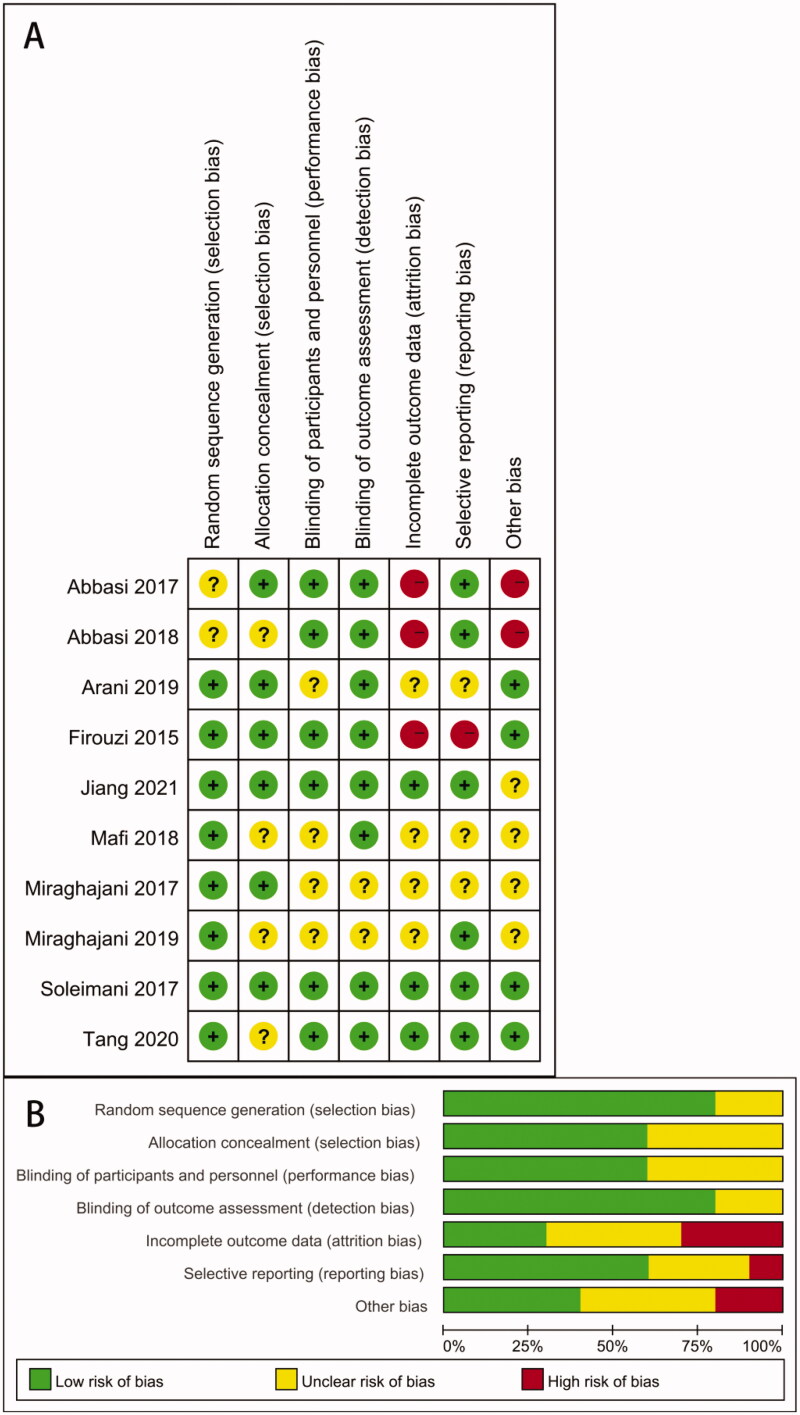
Our analysis revealed that probiotics could delay the progression of renal function injury, improve glucose and lipid metabolism, and reduce inflammation and oxidative stress in patients with DKD. Subgroup analysis showed that intervention duration, probiotic dose and probiotic consumption patterns had an effect of probiotics on outcomes.
益生菌在糖尿病肾病(DKD)管理中的作用已得到证实。目前有几项临床试验正在研究益生菌的作用,益生菌广泛用于调节 DKD 患者肾功能、葡萄糖、脂质、炎症和氧化应激的生物标志物。然而,他们的发现存在争议。本研究旨在系统评价益生菌对 DKD 患者的影响,进行荟萃分析。
从这些数据库建立到 2021 年 9 月,检索 PubMed、The Cochrane Library、Web of Science、Scopus、Embase、中国国家知识基础设施、中国万方数据库和中国 VIP 数据库,以查找相关研究。汇总结果评估了益生菌对 DKD 患者肾功能、葡萄糖、脂质、炎症和氧化应激指标的影响。此外,还分别进行了基于干预持续时间、益生菌剂量和益生菌消费模式的亚组分析。
确定了 10 项包含 552 名参与者的试验进行分析。与对照组相比,益生菌显著降低了血清肌酐(Scr)[WMD=-0.17mg/dL;95%CI=-0.29,-0.05;=0.004]、血尿素氮(BUN)[WMD=-1.36mg/dL;95%CI=-2.20,-0.52;=0.001]、胱抑素 C(Cys C)[WMD=-29.50ng/mL;95%CI=-32.82,-26.18;<0.00001]、尿白蛋白/肌酐比值(UACR)[WMD=-16.05mg/g;95%CI=-27.12,-4.99;=0.004]和钠(Na)[WMD=-0.94mmol/L;95%CI=-1.82,-0.05;=0.04]在 DKD 患者中。与对照组相比,接受益生菌治疗的 DKD 患者血糖控制得到改善,表现为空腹血糖(FPG)、糖化血红蛋白(HbA1c)、稳态模型评估的胰岛素抵抗(HOMA-IR)水平降低,而定量胰岛素敏感性检查指数(QUICKI)升高。益生菌影响脂质代谢参数,降低 DKD 患者的甘油三酯(TG)、总胆固醇(TC)和低密度脂蛋白胆固醇(LDL-c)水平。益生菌还可以通过降低高敏 C 反应蛋白(hs-CRP)、血浆丙二醛(MDA)、总抗氧化能力(TAC)、谷胱甘肽(GSH)和一氧化氮(NO)来改善炎症和氧化应激。此外,亚组分析表明,接受多种益生菌的患者在 BUN、FPG、HOMA-IR、高密度脂蛋白胆固醇(HDL-c)、MDA、TAC 和 NO 方面有统计学差异。同时,当干预持续时间超过 8 周时,Scr、LDL-c、HDL-c、MDA 和 TAC 得到改善,当益生菌剂量大于 40 亿 CFU/天时,BUN、FPG、HOMA-IR 和 MDA 得到改善。
我们的分析表明,益生菌可以延缓肾功能损伤的进展,改善葡萄糖和脂质代谢,降低 DKD 患者的炎症和氧化应激。亚组分析表明,干预持续时间、益生菌剂量和益生菌消费模式对益生菌的作用有影响。