Department of Hepatology, University Hospital Jean Minjoz, Besançon, France.
Department of Cardiology, University Hospital Jean Minjoz, Besançon, France.
PLoS One. 2022 May 26;17(5):e0266965. doi: 10.1371/journal.pone.0266965. eCollection 2022.
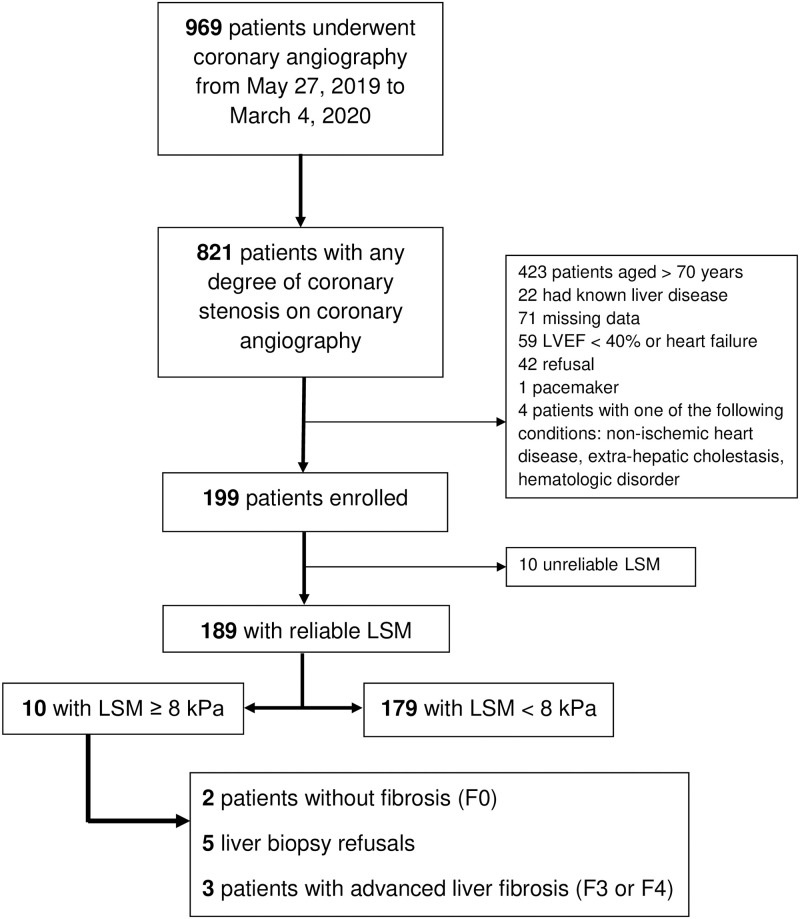
Although coronary artery disease (CAD) and advanced liver fibrosis (AdLF) are commonly associated in patients with non-alcoholic fatty liver disease (NAFLD), the prevalence of AdLF and the diagnostic performance of non-invasive fibrosis tests (NITs) in CAD patients remains unknown. We aimed to prospectively screen for AdLF in patients with documented CAD using NITs and Fibroscan. High and intermediate zones of NITs were combined to define AdLF. AdLF was suspected whenever APRI ≥ 0.5, Forns index ≥ 4.2, NAFLD fibrosis score (NFS) ≥ -1.455/0.12 for age </≥ 65 yrs), Fib4 (≥ 1.30/2.0 for age </≥ 65 yrs) and eLIFT≥ 8. A presumed AdLF assessed by Fibroscan ≥ 8 kPa was the primary outcome measure. Results were given on the basis of intent-to-diagnose liver stiffness ≥ 8 kPa. Among 189 patients (age 60±7years), 10 (5.3%) had a Fibroscan ≥ 8 kPa, of whom 5 underwent liver biopsy (F3/F4: n = 3; no fibrosis: n = 2). AdLF was suspected in 31% of cases using eLIFT (specificity, Sp 70%), 85% with Forns (Sp 16%), 38% with NFS (Sp 63%), 25% with Fib4 (Sp 74%), and 10% with APRI (Sp 91%). In 149 patients "at-risk" of NAFLD (i.e., elevated ALT or diabetes or hypertriglyceridemia or BMI ≥25 kg/m2), AdLF ranged between 10% (APRI) to 84% (Forns). In this subgroup, the most efficient NITs to predict Fibroscan ≥ 8 kPa were eLIFT (Se 60%, Sp 70%) and NFS (Se 70%, Sp 60%). Finally, in CAD patients with risk factors for NAFLD, NFS or the more user-friendly eLIFT are the most attractive first-line biochemical NITs to discriminate good candidates for Fibroscan.
尽管冠状动脉疾病(CAD)和晚期肝纤维化(AdLF)在非酒精性脂肪性肝病(NAFLD)患者中通常同时存在,但 CAD 患者中 AdLF 的患病率和非侵入性纤维化检测(NIT)的诊断性能仍不清楚。我们旨在使用 NIT 和 Fibroscan 前瞻性筛查有记录 CAD 的患者中的 AdLF。将 NIT 的高和中区域结合起来定义 AdLF。只要 APRI≥0.5、Forns 指数≥4.2、NAFLD 纤维化评分(NFS)≥-1.455/0.12(年龄≥65 岁)、Fib4(年龄≥65 岁)≥1.30/2.0)和 eLIFT≥8,就怀疑存在 AdLF。通过 Fibroscan 评估的假定 AdLF≥8kPa 是主要的测量结果。在 189 名患者(年龄 60±7 岁)中,有 10 名(5.3%)Fibroscan≥8kPa,其中 5 名进行了肝活检(F3/F4:n=3;无纤维化:n=2)。使用 eLIFT 怀疑 31%的病例存在 AdLF(特异性,Sp70%),85%使用 Forns(Sp16%),38%使用 NFS(Sp63%),25%使用 Fib4(Sp74%),10%使用 APRI(Sp91%)。在 149 名“有风险”患 NAFLD(即 ALT 升高或糖尿病或高甘油三酯血症或 BMI≥25kg/m2)的患者中,AdLF 介于 10%(APRI)至 84%(Forns)之间。在这个亚组中,预测 Fibroscan≥8kPa 的最有效的 NIT 是 eLIFT(Se60%,Sp70%)和 NFS(Se70%,Sp60%)。最后,在有 NAFLD 危险因素的 CAD 患者中,NFS 或更易用的 eLIFT 是区分 Fibroscan 良好候选者的最有吸引力的一线生化 NIT。