Department of Respiratory Sciences, University of Leicester, Leicester, United Kingdom.
Department of Infection and HIV Medicine, University Hospitals of Leicester NHS Trust, Leicester, United Kingdom.
PLoS Med. 2022 May 26;19(5):e1004015. doi: 10.1371/journal.pmed.1004015. eCollection 2022 May.
Healthcare workers (HCWs), particularly those from ethnic minority groups, have been shown to be at disproportionately higher risk of infection with Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) compared to the general population. However, there is insufficient evidence on how demographic and occupational factors influence infection risk among ethnic minority HCWs.
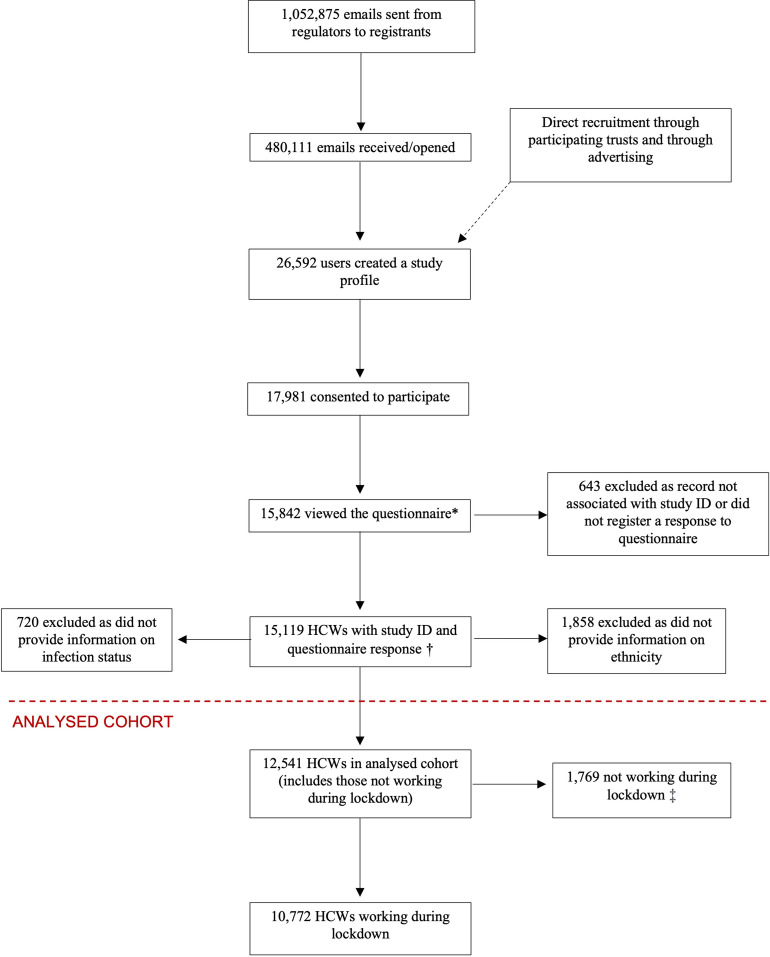
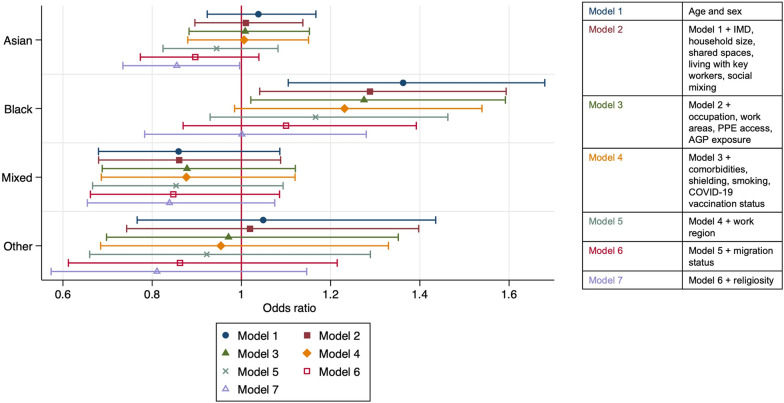
We conducted a cross-sectional analysis using data from the baseline questionnaire of the United Kingdom Research study into Ethnicity and Coronavirus Disease 2019 (COVID-19) Outcomes in Healthcare workers (UK-REACH) cohort study, administered between December 2020 and March 2021. We used logistic regression to examine associations of demographic, household, and occupational risk factors with SARS-CoV-2 infection (defined by polymerase chain reaction (PCR), serology, or suspected COVID-19) in a diverse group of HCWs. The primary exposure of interest was self-reported ethnicity. Among 10,772 HCWs who worked during the first UK national lockdown in March 2020, the median age was 45 (interquartile range [IQR] 35 to 54), 75.1% were female and 29.6% were from ethnic minority groups. A total of 2,496 (23.2%) reported previous SARS-CoV-2 infection. The fully adjusted model contained the following dependent variables: demographic factors (age, sex, ethnicity, migration status, deprivation, religiosity), household factors (living with key workers, shared spaces in accommodation, number of people in household), health factors (presence/absence of diabetes or immunosuppression, smoking history, shielding status, SARS-CoV-2 vaccination status), the extent of social mixing outside of the household, and occupational factors (job role, the area in which a participant worked, use of public transport to work, exposure to confirmed suspected COVID-19 patients, personal protective equipment [PPE] access, aerosol generating procedure exposure, night shift pattern, and the UK region of workplace). After adjustment, demographic and household factors associated with increased odds of infection included younger age, living with other key workers, and higher religiosity. Important occupational risk factors associated with increased odds of infection included attending to a higher number of COVID-19 positive patients (aOR 2.59, 95% CI 2.11 to 3.18 for ≥21 patients per week versus none), working in a nursing or midwifery role (1.30, 1.11 to 1.53, compared to doctors), reporting a lack of access to PPE (1.29, 1.17 to 1.43), and working in an ambulance (2.00, 1.56 to 2.58) or hospital inpatient setting (1.55, 1.38 to 1.75). Those who worked in intensive care units were less likely to have been infected (0.76, 0.64 to 0.92) than those who did not. Black HCWs were more likely to have been infected than their White colleagues, an effect which attenuated after adjustment for other known risk factors. This study is limited by self-selection bias and the cross sectional nature of the study means we cannot infer the direction of causality.
We identified key sociodemographic and occupational risk factors associated with SARS-CoV-2 infection among UK HCWs, and have determined factors that might contribute to a disproportionate odds of infection in HCWs from Black ethnic groups. These findings demonstrate the importance of social and occupational factors in driving ethnic disparities in COVID-19 outcomes, and should inform policies, including targeted vaccination strategies and risk assessments aimed at protecting HCWs in future waves of the COVID-19 pandemic.
The study was prospectively registered at ISRCTN (reference number: ISRCTN11811602).
与一般人群相比,医疗工作者(HCWs),尤其是少数民族群体,感染严重急性呼吸综合征冠状病毒 2 (SARS-CoV-2)的风险更高。然而,关于人口统计学和职业因素如何影响少数民族 HCWs 的感染风险的证据不足。
我们使用英国研究种族和 2019 年冠状病毒疾病(COVID-19)在医疗保健工作者中的结果(UK-REACH)队列研究的基线问卷数据进行了横断面分析,该研究于 2020 年 12 月至 2021 年 3 月之间进行。我们使用逻辑回归来检查人口统计学、家庭和职业危险因素与 SARS-CoV-2 感染(通过聚合酶链反应(PCR)、血清学或疑似 COVID-19 定义)之间的关联,这是一组多样化的 HCWs。主要暴露因素是自我报告的种族。在 2020 年 3 月英国第一次全国封锁期间工作的 10772 名 HCWs 中,中位数年龄为 45 岁(四分位距[IQR] 35 至 54),75.1%为女性,29.6%来自少数民族群体。共有 2496 人(23.2%)报告了以前的 SARS-CoV-2 感染。完全调整后的模型包含以下因变量:人口统计学因素(年龄、性别、种族、移民状况、贫困、宗教信仰)、家庭因素(与关键工作者同住、住宿空间共享、家庭人数)、健康因素(是否存在糖尿病或免疫抑制、吸烟史、是否被隔离、SARS-CoV-2 疫苗接种状况)、家庭外社交混合程度以及职业因素(工作角色、参与者工作的区域、使用公共交通工具上班、接触确诊的疑似 COVID-19 患者、个人防护设备[PPE]的使用情况、气溶胶产生程序的暴露、夜班模式以及工作场所所在的英国地区)。调整后,与感染几率增加相关的人口统计学和家庭因素包括年龄较小、与其他关键工作者同住以及宗教信仰更高。与感染几率增加相关的重要职业危险因素包括照顾更多 COVID-19 阳性患者(每周≥21 名患者的比值比[OR]为 2.59,95%置信区间[CI]为 2.11 至 3.18,而无患者)、从事护理或助产工作(1.30,1.11 至 1.53,与医生相比)、报告缺乏 PPE (1.29,1.17 至 1.43)、在救护车(2.00,1.56 至 2.58)或医院住院环境(1.55,1.38 至 1.75)工作。与未感染者相比,在重症监护病房工作的 HCWs 感染的可能性较低(0.76,0.64 至 0.92)。黑人 HCWs 比白人同事更有可能感染,这种影响在调整其他已知危险因素后减弱。本研究受到自我选择偏倚的限制,且研究的横断面性质意味着我们无法推断因果关系的方向。
我们确定了与英国 HCWs 中 SARS-CoV-2 感染相关的关键社会人口统计学和职业危险因素,并确定了可能导致黑人族裔 HCWs 感染几率不成比例的因素。这些发现表明,社会和职业因素在推动 COVID-19 结果的种族差异方面的重要性,并应指导政策,包括有针对性的疫苗接种策略和风险评估,以保护未来 COVID-19 大流行中的 HCWs。
该研究在 ISRCTN(参考号:ISRCTN82536652)进行了前瞻性注册。