Murtha-Lemekhova Anastasia, Fuchs Juri, Teroerde Miriam, Chiriac Ute, Klotz Rosa, Hornuss Daniel, Larmann Jan, Weigand Markus A, Hoffmann Katrin
Department of General, Visceral and Transplantation Surgery, Heidelberg University Hospital, 69120 Heidelberg, Germany.
Department of Pharmacy, Heidelberg University Hospital, 69120 Heidelberg, Germany.
Antibiotics (Basel). 2022 May 12;11(5):649. doi: 10.3390/antibiotics11050649.
Prophylactic antibiotics are frequently administered after major abdominal surgery including hepatectomies aiming to prevent infective complications. Yet, excessive use of antibiotics increases resistance in bacteria. The aim of this systematic review and meta-analysis is to assess the efficacy of prophylactic antibiotics after hepatectomy (postoperative antibiotic prophylaxis, POA).
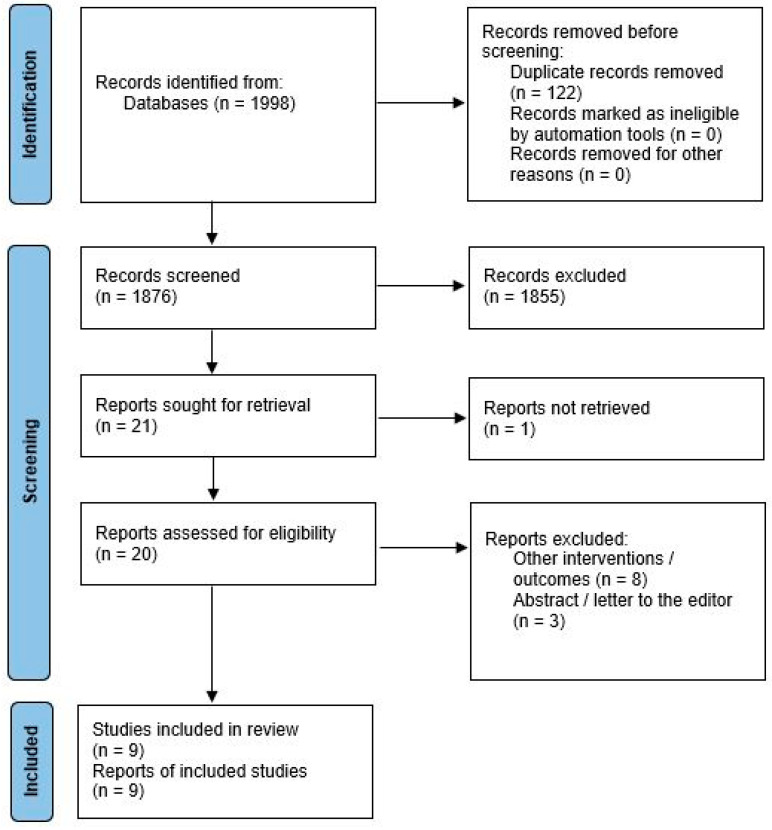
This systematic review and meta-analysis were completed according to the current PRISMA guidelines. The protocol has been registered prior to data extraction (PROSPERO registration Nr: CRD42021288510). MEDLINE, Web of Science and CENTRAL were searched for clinical reports on POA in hepatectomy restrictions. A random-effects model was used for synthesis. Methodological quality was assessed with RoB2 and ROBINS-I. GRADE was used for the quality of evidence assessment.
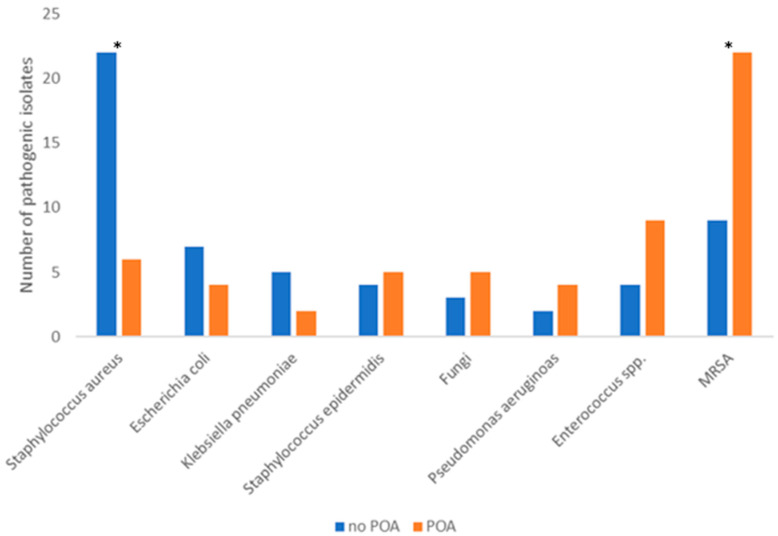
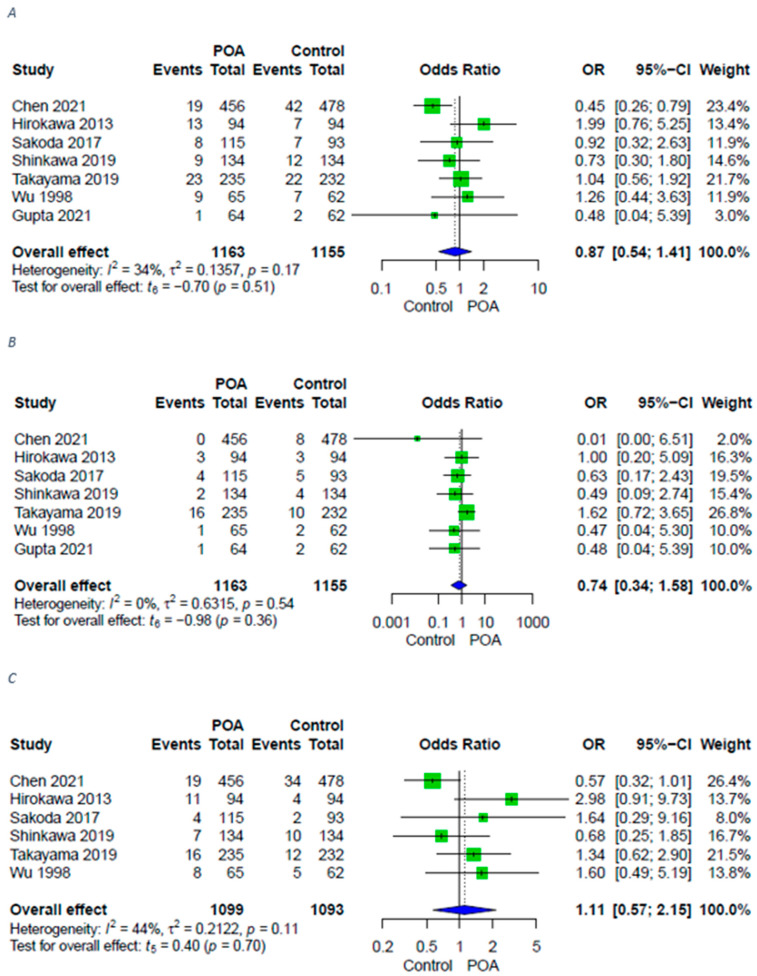
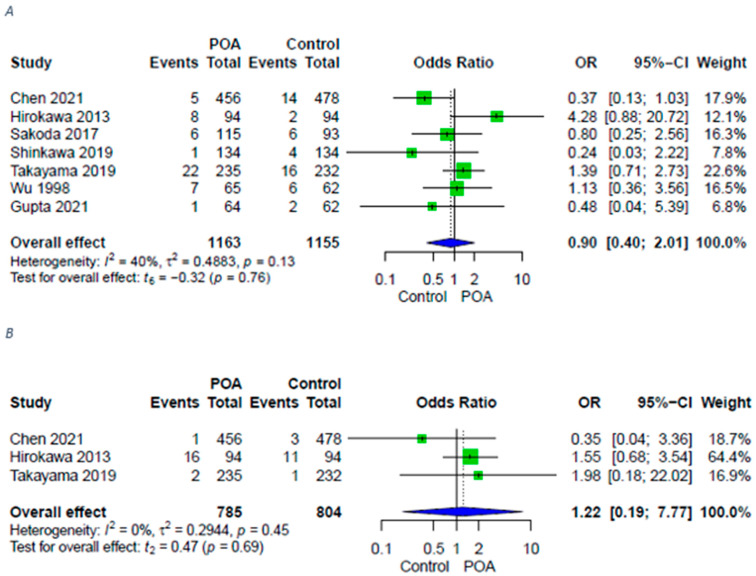
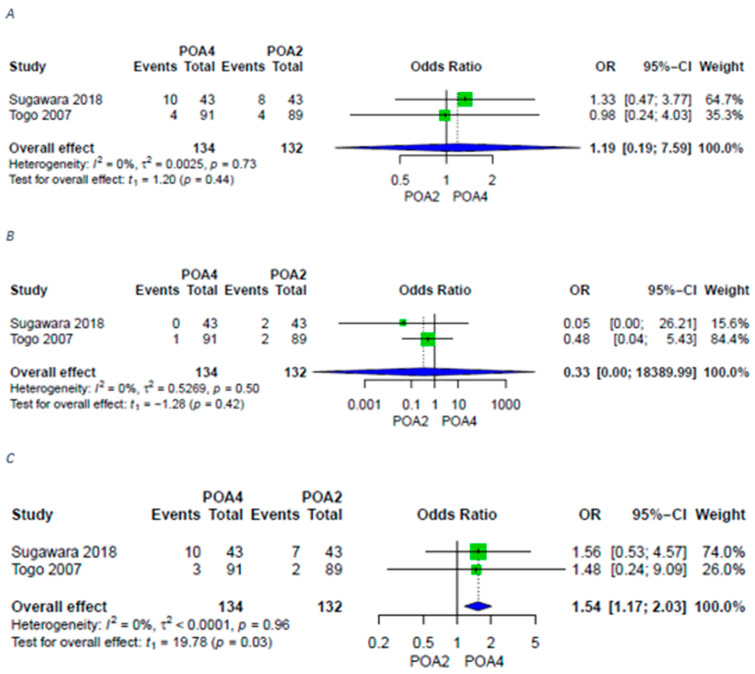
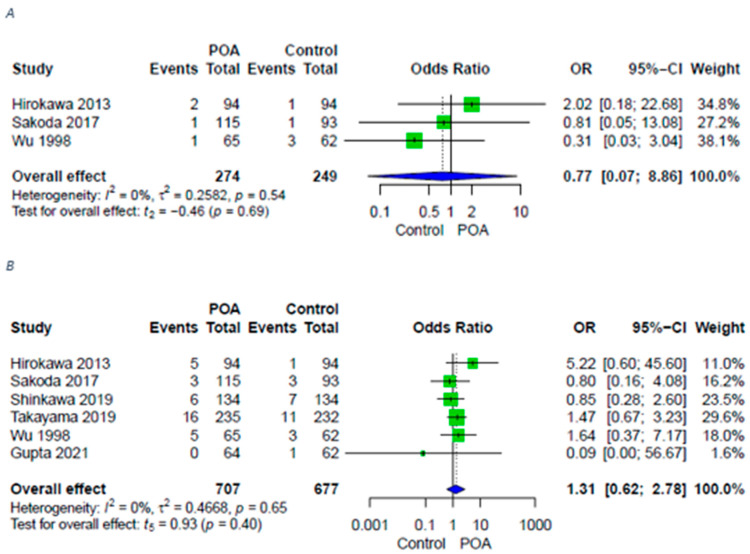
Nine comparative studies comprising 2987 patients were identified: six randomized controlled trials (RCTs) and three retrospectives. POA did not lead to a reduction in postoperative infective complications or have an effect on liver-specific complications-post-hepatectomy liver failure and biliary leaks. POA over four or more days was associated with increased rates of deep surgical site infections compared to short-term administration for up to two days (OR 1.54; 95% CI [1.17;2.03]; = 0.03). Routine POA led to significantly higher MRSA incidence as a pathogen ( = 0.0073). Overall, the risk of bias in the studies was low and the quality of evidence moderate.
Routine POA cannot be recommended after hepatectomy since it does not reduce postoperative infection or liver-specific complications but contributes to resistance in bacteria. Studies into individualized risk-adapted antibiotic prophylaxis strategies are needed to further optimize perioperative treatment in liver surgery.
预防性抗生素常用于包括肝切除术在内的腹部大手术后,旨在预防感染性并发症。然而,抗生素的过度使用会增加细菌耐药性。本系统评价和荟萃分析的目的是评估肝切除术后预防性抗生素(术后抗生素预防,POA)的疗效。
本系统评价和荟萃分析按照当前PRISMA指南完成。方案在数据提取前已注册(PROSPERO注册号:CRD42021288510)。检索MEDLINE、科学网和CENTRAL,查找关于肝切除术限制下POA的临床报告。采用随机效应模型进行综合分析。使用RoB2和ROBINS-I评估方法学质量。使用GRADE评估证据质量。
确定了9项比较研究,共2987例患者:6项随机对照试验(RCT)和3项回顾性研究。POA并未导致术后感染性并发症减少,也未对肝特异性并发症——肝切除术后肝功能衰竭和胆漏产生影响。与短期使用最多2天相比,POA使用4天或更长时间与深部手术部位感染率增加相关(OR 1.54;95%CI[1.17;2.03];P = 0.03)。常规POA导致作为病原体的耐甲氧西林金黄色葡萄球菌(MRSA)发生率显著更高(P = 0.0073)。总体而言,研究中的偏倚风险较低,证据质量中等。
肝切除术后不建议常规使用POA,因为它不能降低术后感染或肝特异性并发症,但会导致细菌耐药。需要开展针对个体化风险适应性抗生素预防策略的研究,以进一步优化肝脏手术的围手术期治疗。