Wellcome Centre for Infectious Diseases Research in Africa, Institute of Infectious Disease and Molecular Medicine, University of Cape Town, Cape Town, South Africa; Department of Medicine, University of Cape Town, Cape Town, South Africa.
Wellcome Centre for Infectious Diseases Research in Africa, Institute of Infectious Disease and Molecular Medicine, University of Cape Town, Cape Town, South Africa; Department of Medicine, University of Cape Town, Cape Town, South Africa.
Lancet Microbe. 2022 Jul;3(7):e521-e532. doi: 10.1016/S2666-5247(22)00062-3. Epub 2022 May 26.
Mycobacterium tuberculosis bloodstream infection is a leading cause of death in people living with HIV and disseminated bacillary load might be a key driver of disease severity. We aimed to assess Xpert MTB/RIF Ultra (Xpert Ultra) testing of blood as a diagnostic for M tuberculosis bloodstream infection and investigate cycle threshold as a quantitative disease biomarker.
In this cohort study, we obtained biobanked blood samples from a large and well characterised cohort of adult patients admitted to hospital in Western Cape, South Africa with suspected HIV-associated tuberculosis and a CD4 count less than 350 cells per μL. Patients already receiving antituberculosis therapy were excluded. Samples were obtained on recruitment within 72 h of admission to hospital, and patients were followed up for 12 weeks to determine survival. We tested the biobanked blood samples using the Xpert Ultra platform after lysis and wash processing of the blood. We assessed diagnostic yield (proportion of cases detected, with unavailable test results coded as negative) against a microbiological reference, both as a function of markers of critical-illness and compared with other rapid diagnostics (urine lipoarabinomannan and sputum Xpert). Quantitative blood Xpert Ultra results were evaluated as a disease biomarker by assessing association with disease phenotype defined by principal component analysis of 32 host-response markers. Prognostic value compared to other tuberculosis biomarkers was assessed using likelihood ratio testing of nested models predicting 12-week mortality.
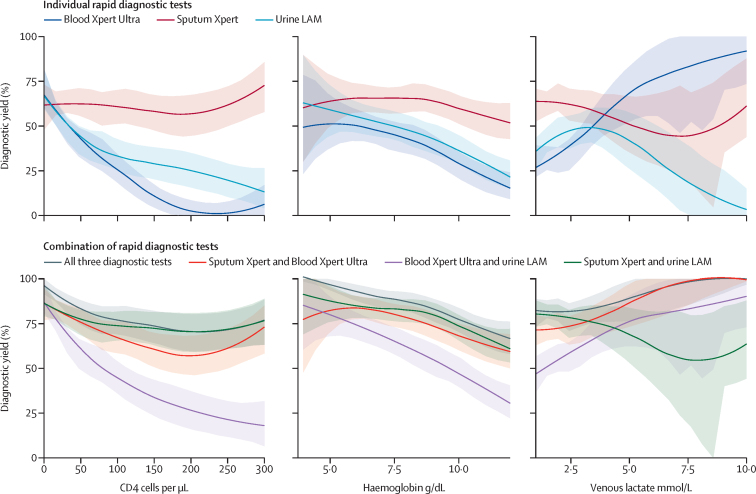
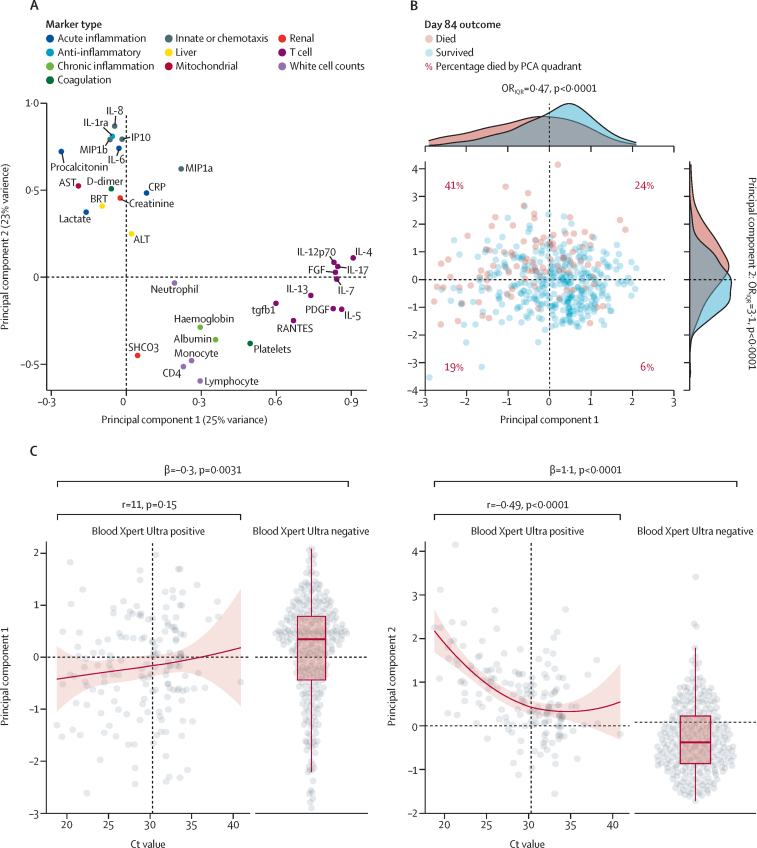
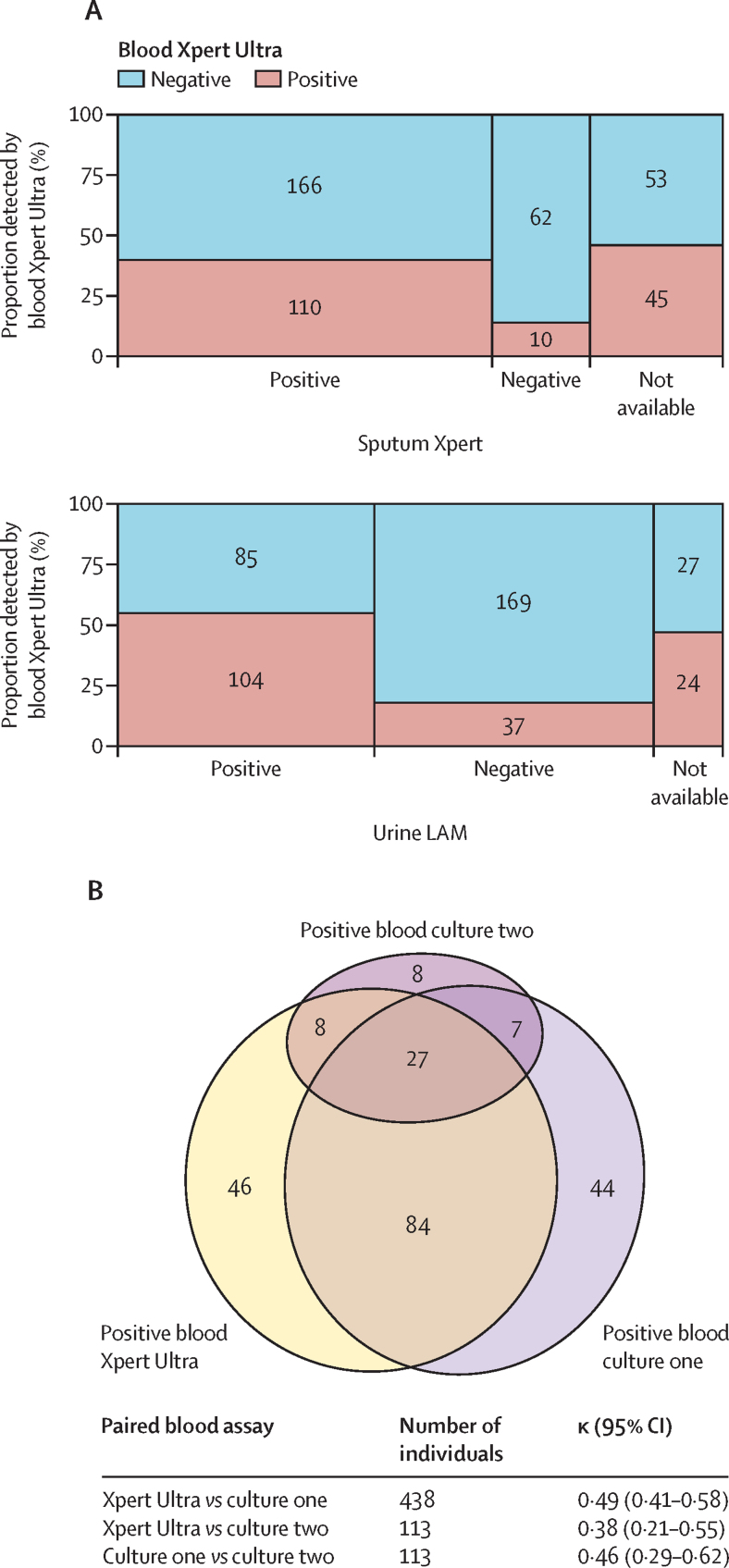
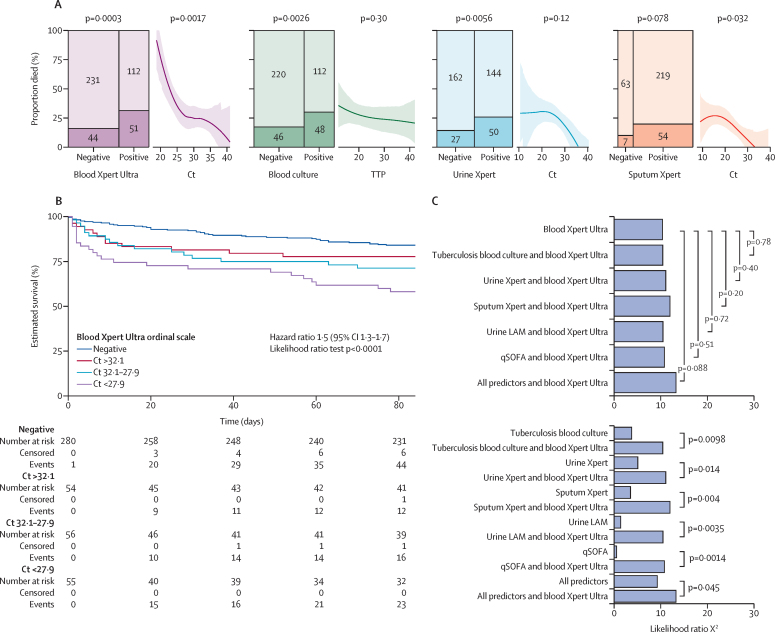
Between Jan 16, 2014, and Oct 19, 2016, of the 659 participants recruited to the parent study, 582 had an available biobanked blood sample. 447 (77%) of 582 met the microbiological reference standard for tuberculosis diagnosis. Median CD4 count was 62 (IQR 221-33) cells per μL, and 123 (21%) of participants died by 12-weeks follow-up. Blood Xpert Ultra was positive in 165 (37%) of 447 participants with confirmed tuberculosis by the microbiological reference standard, with a diagnostic yield of 0·37 (95% CI 0·32-0·42). Diagnostic yield increased with lower CD4 count or haemoglobin, and outperformed urine lipoarabinomannan testing in participants with elevated venous lactate. Quantitative blood Xpert Ultra results were more closely associated with mortality than other tuberculosis biomarkers including blood culture, and urine lipoarabinomannan, or urine Xpert (all p<0·05). A principal component of clinical phenotype capturing markers of inflammation, tissue damage, and organ dysfunction was strongly associated with both blood Xpert-Ultra positivity (associated with a SD increase of 1·1 in PC score, p<0·0001) and cycle threshold (r= -0·5; p<0·0001).
Xpert Ultra testing of pre-processed blood could be used as a rapid diagnostic test in critically ill patients with suspected HIV-associated tuberculosis, while also giving additional prognostic information compared with other available markers. A dose-response relationship between quantitative blood Xpert Ultra results, host-response phenotype, and mortality risk adds to evidence that suggests M tuberculosis bloodstream infection bacillary load is causally related to outcomes.
Wellcome Trust, National Institute of Health Fogarty International Center, South African MRC, UK National Institute of Health Research, National Research Foundation of South Africa.
For the Xhosa and Afrikaans translations of the abstract see Supplementary Materials section.
结核分枝杆菌血流感染是导致 HIV 感染者死亡的主要原因,播散性细菌负荷可能是疾病严重程度的关键驱动因素。本研究旨在评估 Xpert MTB/RIF Ultra(Xpert Ultra)检测血液作为结核分枝杆菌血流感染的诊断方法,并研究循环阈值作为疾病的定量生物标志物。
在这项队列研究中,我们从南非西开普省一家大型且特征明确的成年疑似 HIV 相关结核病患者队列中获取了生物银行血液样本,这些患者的 CD4 计数小于 350 个细胞/μL。已接受抗结核治疗的患者被排除在外。在入院后 72 小时内采集样本,并在 12 周内进行随访以确定患者的生存情况。我们使用 Xpert Ultra 平台对采集的生物银行血液样本进行检测,检测前对血液进行裂解和洗涤处理。我们评估了诊断率(检测到的病例比例,无法获得检测结果的病例编码为阴性)与微生物学参考标准的相关性,同时评估了与其他快速诊断检测方法(尿液脂阿拉伯甘露聚糖和痰液 Xpert)的相关性。通过对 32 个宿主反应标志物的主成分分析定义疾病表型,评估定量血液 Xpert Ultra 结果作为疾病标志物的价值。使用嵌套模型的似然比检验评估其与其他结核病生物标志物的预后价值,这些模型用于预测 12 周死亡率。
在 2014 年 1 月 16 日至 2016 年 10 月 19 日期间,在参加母研究的 659 名参与者中,582 名有可用的生物银行血液样本。447(77%)名符合结核病微生物学参考标准。中位 CD4 计数为 62(221-33)个细胞/μL,123 名(21%)参与者在 12 周随访时死亡。在 447 名符合微生物学参考标准的结核病患者中,165 名(37%)的血液 Xpert Ultra 检测结果为阳性,诊断率为 0.37(95%CI 0.32-0.42)。诊断率随 CD4 计数或血红蛋白降低而增加,在静脉乳酸水平升高的患者中,优于尿液脂阿拉伯甘露聚糖检测。定量血液 Xpert Ultra 结果与其他结核病生物标志物(包括血液培养、尿液脂阿拉伯甘露聚糖或尿液 Xpert)相比,与死亡率的相关性更强(均 P<0.05)。反映炎症、组织损伤和器官功能障碍的临床表型的主要成分与血液 Xpert-Ultra 阳性(与 PC 评分增加 1.1 相关,P<0.0001)和循环阈值(r=-0.5;P<0.0001)均具有很强的相关性。
经过预处理的血液 Xpert Ultra 检测可作为疑似 HIV 相关结核病危重症患者的快速诊断检测方法,与其他现有标志物相比,还能提供额外的预后信息。定量血液 Xpert Ultra 结果、宿主反应表型与死亡率风险之间的剂量-反应关系进一步证明了结核分枝杆菌血流感染细菌负荷与结局之间存在因果关系。
英国惠康信托基金会、美国国立卫生研究院福格蒂国际中心、南非医学研究理事会、英国国家卫生研究院、南非国家研究基金会。