Department of Healthcare Epidemiology, School of Public Health in the Graduate School of Medicine, Kyoto University, Kyoto, Japan.
Department of Intensive Care Medicine, Kameda Medical Center, 929 Higashi-cho, Kamogawa, Chiba, Japan.
Sci Rep. 2022 Jun 4;12(1):9331. doi: 10.1038/s41598-022-13224-y.
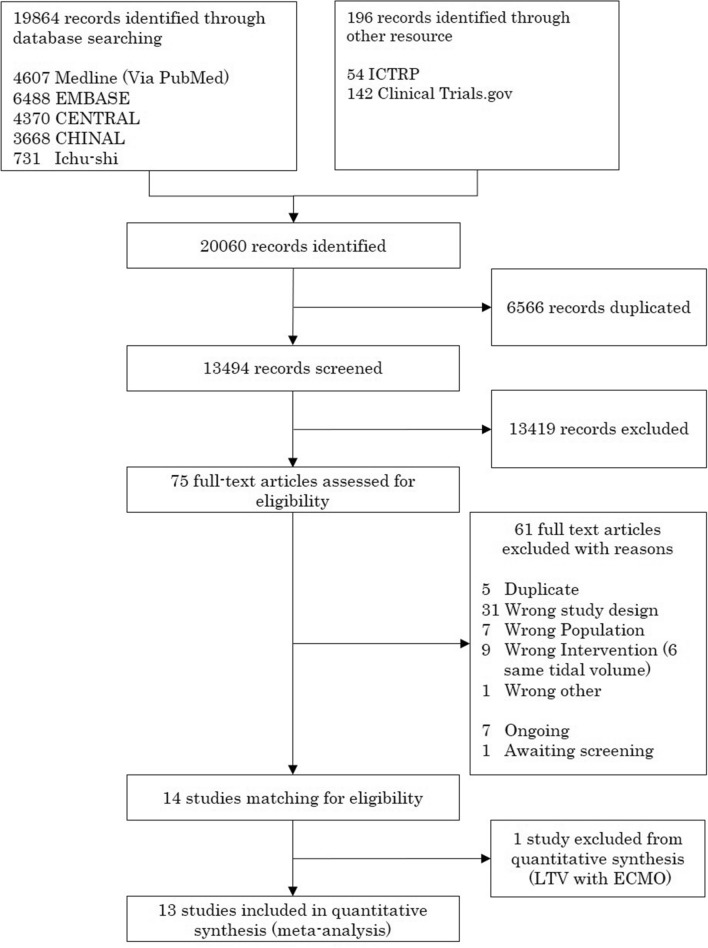
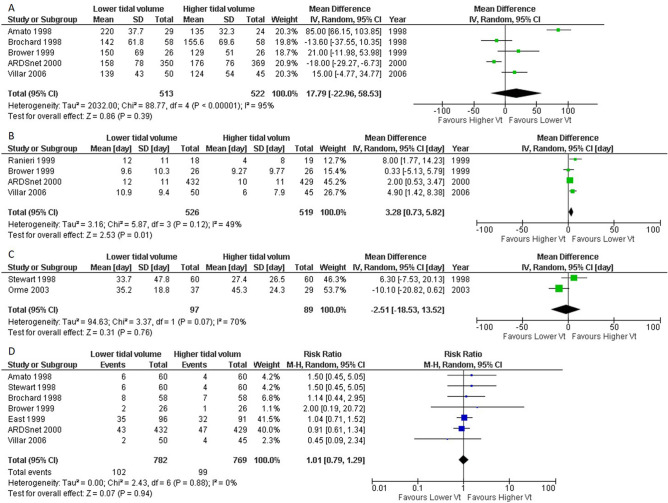
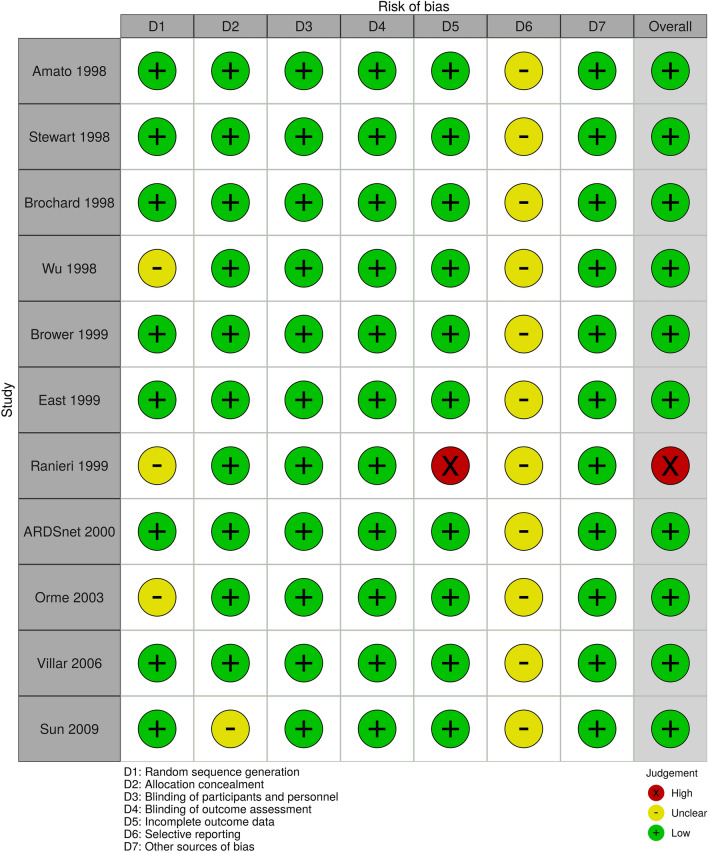
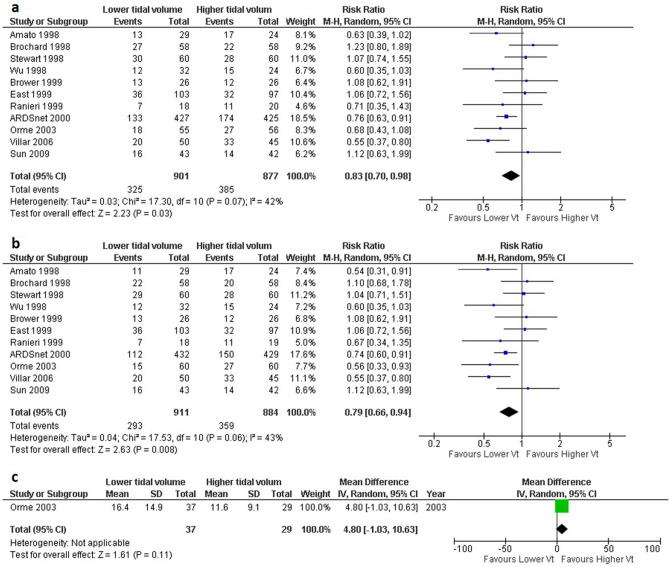
The effects of lower tidal volume ventilation (LTV) were controversial for patients with acute respiratory distress syndrome (ARDS). This systematic review and meta-analysis aimed to evaluate the use of LTV strategy in patients with ARDS. We performed a literature search on MEDLINE, CENTRAL, EMBASE, CINAHL, "Igaku-Chuo-Zasshi", clinical trial registration sites, and the reference of recent guidelines. We included randomized controlled trials (RCTs) to compare the LTV strategy with the higher tidal volume ventilation (HTV) strategy in patients with ARDS. Two authors independently evaluated the eligibility of studies and extracted the data. The primary outcomes were 28-day mortality. We used the GRADE methodology to assess the certainty of evidence. Among the 19,864 records screened, 13 RCTs that recruited 1874 patients were included in our meta-analysis. When comparing LTV (4-8 ml/kg) versus HTV (> 8 ml/kg), the pooled risk ratio for 28-day mortality was 0.79 (11 studies, 95% confidence interval [CI] 0.66-0.94, I = 43%, n = 1795, moderate certainty of evidence). Subgroup-analysis by combined high positive end-expiratory pressure with LTV showed interaction (P = 0.01). Our study indicated that ventilation with LTV was associated with reduced risk of mortality in patients with ARDS when compared with HTV. Trial registration: UMIN-CTR (UMIN000041071).
低潮气量通气(LTV)对急性呼吸窘迫综合征(ARDS)患者的影响存在争议。本系统评价和荟萃分析旨在评估 LTV 策略在 ARDS 患者中的应用。我们在 MEDLINE、CENTRAL、EMBASE、CINAHL、"Igaku-Chuo-Zasshi"、临床试验注册网站和最近指南的参考文献中进行了文献检索。我们纳入了比较 LTV 策略与高潮气量通气(HTV)策略在 ARDS 患者中的随机对照试验(RCT)。两位作者独立评估了研究的纳入标准并提取了数据。主要结局为 28 天死亡率。我们使用 GRADE 方法评估证据的确定性。在筛选的 19864 条记录中,有 13 项 RCT 共纳入 1874 名患者纳入我们的荟萃分析。与 HTV(>8ml/kg)相比,LTV(4-8ml/kg)组的 28 天死亡率的汇总风险比为 0.79(11 项研究,95%置信区间[CI] 0.66-0.94,I=43%,n=1795,中等确定性证据)。与 LTV 联合高呼气末正压的亚组分析显示存在交互作用(P=0.01)。我们的研究表明,与 HTV 相比,ARDS 患者采用 LTV 通气可降低死亡率风险。试验注册:UMIN-CTR(UMIN000041071)。