Hanson Sarah Wulf, Abbafati Cristiana, Aerts Joachim G, Al-Aly Ziyad, Ashbaugh Charlie, Ballouz Tala, Blyuss Oleg, Bobkova Polina, Bonsel Gouke, Borzakova Svetlana, Buonsenso Danilo, Butnaru Denis, Carter Austin, Chu Helen, De Rose Cristina, Diab Mohamed Mustafa, Ekbom Emil, El Tantawi Maha, Fomin Victor, Frithiof Robert, Gamirova Aysylu, Glybochko Petr V, Haagsma Juanita A, Javanmard Shaghayegh Haghjooy, Hamilton Erin B, Harris Gabrielle, Heijenbrok-Kal Majanka H, Helbok Raimund, Hellemons Merel E, Hillus David, Huijts Susanne M, Hultström Michael, Jassat Waasila, Kurth Florian, Larsson Ing-Marie, Lipcsey Miklós, Liu Chelsea, Loflin Callan D, Malinovschi Andrei, Mao Wenhui, Mazankova Lyudmila, McCulloch Denise, Menges Dominik, Mohammadifard Noushin, Munblit Daniel, Nekliudov Nikita A, Ogbuoji Osondu, Osmanov Ismail M, Peñalvo José L, Petersen Maria Skaalum, Puhan Milo A, Rahman Mujibur, Rass Verena, Reinig Nickolas, Ribbers Gerard M, Ricchiuto Antonia, Rubertsson Sten, Samitova Elmira, Sarrafzadegan Nizal, Shikhaleva Anastasia, Simpson Kyle E, Sinatti Dario, Soriano Joan B, Spiridonova Ekaterina, Steinbeis Fridolin, Svistunov Andrey A, Valentini Piero, van de Water Brittney J, van den Berg-Emons Rita, Wallin Ewa, Witzenrath Martin, Wu Yifan, Xu Hanzhang, Zoller Thomas, Adolph Christopher, Albright James, Amlag Joanne O, Aravkin Aleksandr Y, Bang-Jensen Bree L, Bisignano Catherine, Castellano Rachel, Castro Emma, Chakrabarti Suman, Collins James K, Dai Xiaochen, Daoud Farah, Dapper Carolyn, Deen Amanda, Duncan Bruce B, Erickson Megan, Ewald Samuel B, Ferrari Alize J, Flaxman Abraham D, Fullman Nancy, Gamkrelidze Amiran, Giles John R, Guo Gaorui, Hay Simon I, He Jiawei, Helak Monika, Hulland Erin N, Kereselidze Maia, Krohn Kris J, Lazzar-Atwood Alice, Lindstrom Akiaja, Lozano Rafael, Magistro Beatrice, Malta Deborah Carvalho, Månsson Johan, Herrera Ana M Mantilla, Mokdad Ali H, Monasta Lorenzo, Nomura Shuhei, Pasovic Maja, Pigott David M, Reiner Robert C, Reinke Grace, Ribeiro Antonio Luiz P, Santomauro Damian Francesco, Sholokhov Aleksei, Spurlock Emma Elizabeth, Walcott Rebecca, Walker Ally, Wiysonge Charles Shey, Zheng Peng, Bettger Janet Prvu, Murray Christopher Jl, Vos Theo
Institute for Health Metrics and Evaluation, University of Washington, Seattle, WA, USA.
Department of Juridical and Economic Studies, La Sapienza University, Rome, Italy.
medRxiv. 2022 May 27:2022.05.26.22275532. doi: 10.1101/2022.05.26.22275532.
While much of the attention on the COVID-19 pandemic was directed at the daily counts of cases and those with serious disease overwhelming health services, increasingly, reports have appeared of people who experience debilitating symptoms after the initial infection. This is popularly known as long COVID.
To estimate by country and territory of the number of patients affected by long COVID in 2020 and 2021, the severity of their symptoms and expected pattern of recovery.
We jointly analyzed ten ongoing cohort studies in ten countries for the occurrence of three major symptom clusters of long COVID among representative COVID cases. The defining symptoms of the three clusters (fatigue, cognitive problems, and shortness of breath) are explicitly mentioned in the WHO clinical case definition. For incidence of long COVID, we adopted the minimum duration after infection of three months from the WHO case definition. We pooled data from the contributing studies, two large medical record databases in the United States, and findings from 44 published studies using a Bayesian meta-regression tool. We separately estimated occurrence and pattern of recovery in patients with milder acute infections and those hospitalized. We estimated the incidence and prevalence of long COVID globally and by country in 2020 and 2021 as well as the severity-weighted prevalence using disability weights from the Global Burden of Disease study.
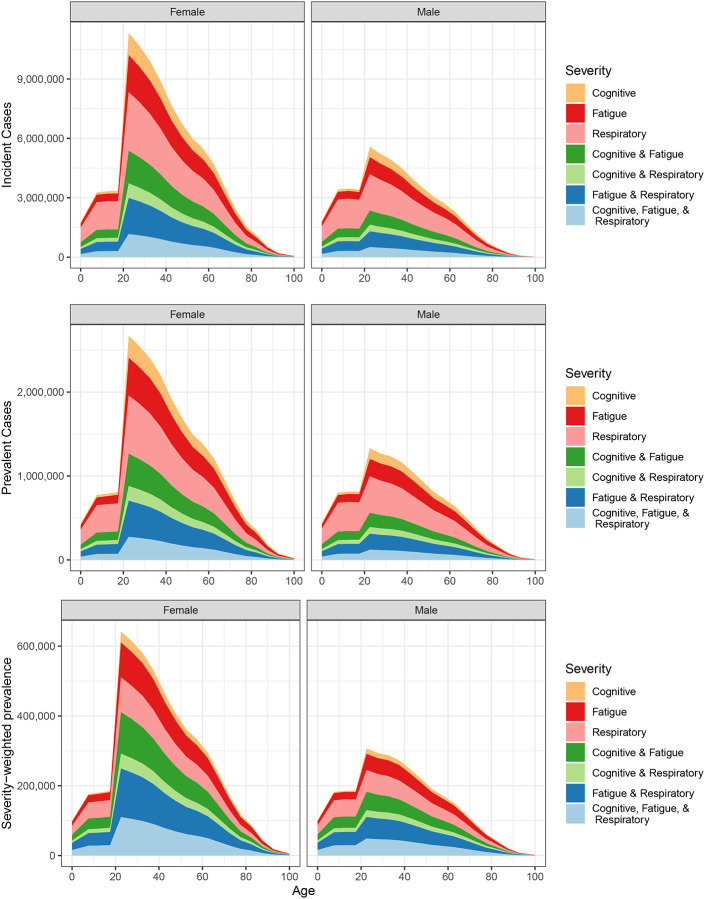
Analyses are based on detailed information for 1906 community infections and 10526 hospitalized patients from the ten collaborating cohorts, three of which included children. We added published data on 37262 community infections and 9540 hospitalized patients as well as ICD-coded medical record data concerning 1.3 million infections. Globally, in 2020 and 2021, 144.7 million (95% uncertainty interval [UI] 54.8-312.9) people suffered from any of the three symptom clusters of long COVID. This corresponds to 3.69% (1.38-7.96) of all infections. The fatigue, respiratory, and cognitive clusters occurred in 51.0% (16.9-92.4), 60.4% (18.9-89.1), and 35.4% (9.4-75.1) of long COVID cases, respectively. Those with milder acute COVID-19 cases had a quicker estimated recovery (median duration 3.99 months [IQR 3.84-4.20]) than those admitted for the acute infection (median duration 8.84 months [IQR 8.10-9.78]). At twelve months, 15.1% (10.3-21.1) continued to experience long COVID symptoms.
The occurrence of debilitating ongoing symptoms of COVID-19 is common. Knowing how many people are affected, and for how long, is important to plan for rehabilitative services and support to return to social activities, places of learning, and the workplace when symptoms start to wane.
What are the extent and nature of the most common long COVID symptoms by country in 2020 and 2021? Globally, 144.7 million people experienced one or more of three symptom clusters (fatigue; cognitive problems; and ongoing respiratory problems) of long COVID three months after infection, in 2020 and 2021. Most cases arose from milder infections. At 12 months after infection, 15.1% of these cases had not yet recovered. The substantial number of people with long COVID are in need of rehabilitative care and support to transition back into the workplace or education when symptoms start to wane.
在新冠疫情期间,大部分注意力都集中在每日新增病例数以及那些病情严重、使医疗服务不堪重负的患者身上,但越来越多的报告显示,有些人在初次感染后出现了使人衰弱的症状。这就是通常所说的“长新冠”。
按国家和地区估算2020年和2021年受“长新冠”影响的患者数量、症状严重程度以及预期的康复模式。
我们联合分析了十个国家正在进行的十项队列研究,以了解具有代表性的新冠病例中“长新冠”的三个主要症状群的发生情况。世界卫生组织的临床病例定义中明确提到了这三个症状群的定义症状(疲劳、认知问题和呼吸急促)。对于“长新冠”的发病率,我们采用了世界卫生组织病例定义中感染后至少三个月的最短持续时间。我们使用贝叶斯元回归工具汇总了参与研究、美国两个大型医疗记录数据库的数据以及44项已发表研究的结果。我们分别估计了轻度急性感染患者和住院患者的发病情况及康复模式。我们估计了2020年和2021年全球及各国“长新冠”的发病率和患病率,以及使用全球疾病负担研究中的残疾权重得出的严重程度加权患病率。
分析基于十个合作队列中1906例社区感染和10526例住院患者的详细信息,其中三个队列包括儿童。我们还添加了37262例社区感染和9540例住院患者的已发表数据,以及涉及130万例感染的国际疾病分类编码医疗记录数据。在全球范围内,2020年和2021年,有1.447亿人(95%不确定区间[UI]为5480万 - 3.129亿)出现了“长新冠”的三个症状群中的任何一个。这相当于所有感染病例的3.69%(1.38% - 7.96%)。在“长新冠”病例中,疲劳、呼吸和认知症状群分别出现在51.0%(16.9% - 92.4%)、60.4%(18.9% - 89.1%)和35.4%(9.4% - 75.1%)的患者中。急性新冠病情较轻的患者预计恢复得更快(中位持续时间3.99个月[IQR 3.84 - 4.20]),而因急性感染入院的患者恢复时间较长(中位持续时间8.84个月[IQR 8.10 - 9.78])。在感染十二个月后,15.1%(10.3% - 21.1%)的患者仍有“长新冠”症状。
新冠病毒感染后出现使人衰弱的持续症状很常见。了解受影响的人数以及持续时间,对于规划康复服务以及在症状开始缓解时支持患者重返社交活动、学习场所和工作场所非常重要。
2020年和2021年各国最常见的“长新冠”症状的范围和性质是什么?在全球范围内,2020年和2021年,1.447亿人在感染三个月后出现了“长新冠”的三个症状群中的一个或多个(疲劳、认知问题和持续的呼吸问题)。大多数病例来自病情较轻的感染。在感染十二个月后,15.1%的这些病例尚未康复。大量“长新冠”患者在症状开始缓解时需要康复护理和支持,以便重返工作岗位或继续接受教育。